

Bone Health After Bariatric Surgery
- PMID: 30283897
- PMCID: PMC6124196
- DOI: 10.1002/jbm4.10048
Bone Health After Bariatric Surgery
Abstract
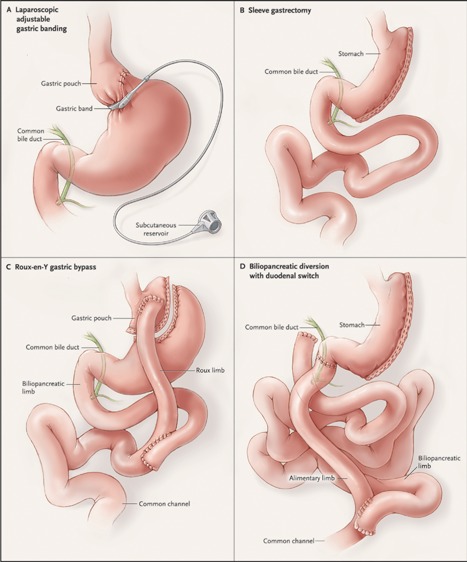
Bariatric surgery results in long-term weight loss and improvement or resolution in obesity-related comorbidities. However, mounting evidence indicates that it adversely affects bone health. This review summarizes clinical research findings about the impact of bariatric surgery on skeletal outcomes. The literature is the largest and strongest for the Roux-en-Y gastric bypass (RYGB) procedure, as RYGB was the most commonly performed bariatric procedure worldwide until it was very recently overtaken by the sleeve gastrectomy (SG). Because SG is a newer procedure, its skeletal effects have not yet been well defined. Epidemiologic studies have now demonstrated an increased risk of fracture after RYGB and biliopancreatic diversion with duodenal switch, both of which include a malabsorptive component. As these epidemiologic data have emerged, patient-oriented studies have elucidated the bone tissue-level changes that may account for the heightened skeletal fragility. Bariatric surgery induces early and dramatic increases in biochemical markers of bone turnover. A notable feature of recent patient-oriented clinical studies is the application of advanced skeletal imaging modalities; studies address the limitations of dual-energy X-ray absorptiometry (DXA) by using quantitative computed tomography (QCT)-based modalities to examine volumetric bone mineral density and compartment-specific density and microstructure. RYGB results in pronounced declines in bone mass at the axial skeleton demonstrated by DXA and QCT, as well as at the appendicular skeleton demonstrated by high-resolution peripheral quantitative computed tomography (HR-pQCT). RYGB has detrimental effects on trabecular and cortical microarchitecture and estimated bone strength. Skeletal changes after RYGB appear early and continue even after weight loss plateaus and weight stabilizes. The skeletal effects of bariatric surgery are presumably multifactorial, and mechanisms may involve nutritional factors, mechanical unloading, hormonal factors, and changes in body composition and bone marrow fat. Clinical guidelines address bone health and may mitigate the negative skeletal effects of surgery, although more research is needed to direct and support such guidelines. © 2018 The Authors. JBMR Plus is published by Wiley Periodicals, Inc. on behalf of American Society for Bone and Mineral Research.
Keywords: BIOCHEMICAL MARKERS OF BONE TURNOVER; BONE QCT/μCT; BONE–FAT INTERACTIONS; DXA; FRACTURE RISK ASSESSMENT.
Figures
References
-
- Non‐communicable Disease Risk Factor Collaboration. Worldwide trends in body‐mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population‐based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 2017; 390:2627–42. - PMC - PubMed
-
- Crawford MR, Pham N, Khan L, Bena JF, Schauer PR, Kashyap SR. Increased bone turnover in type 2 diabetes patients randomized to bariatric surgery vs. medical therapy at least 5 years. Endocr Pract. Epub 2017. Nov 16. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials