

Outcomes of Patients With Asymptomatic Aortic Stenosis Followed Up in Heart Valve Clinics
- PMID: 30285058
- PMCID: PMC6583052
- DOI: 10.1001/jamacardio.2018.3152
Outcomes of Patients With Asymptomatic Aortic Stenosis Followed Up in Heart Valve Clinics
Abstract
Importance: The natural history and the management of patients with asymptomatic aortic stenosis (AS) have not been fully examined in the current era.
Objective: To determine the clinical outcomes of patients with asymptomatic AS using data from the Heart Valve Clinic International Database.
Design, setting, and participants: This registry was assembled by merging data from prospectively gathered institutional databases from 10 heart valve clinics in Europe, Canada, and the United States. Asymptomatic patients with an aortic valve area of 1.5 cm2 or less and preserved left ventricular ejection fraction (LVEF) greater than 50% at entry were considered for the present analysis. Data were collected from January 2001 to December 2014, and data were analyzed from January 2017 to July 2018.
Main outcomes and measures: Natural history, need for aortic valve replacement (AVR), and survival of asymptomatic patients with moderate or severe AS at entry followed up in a heart valve clinic. Indications for AVR were based on current guideline recommendations.
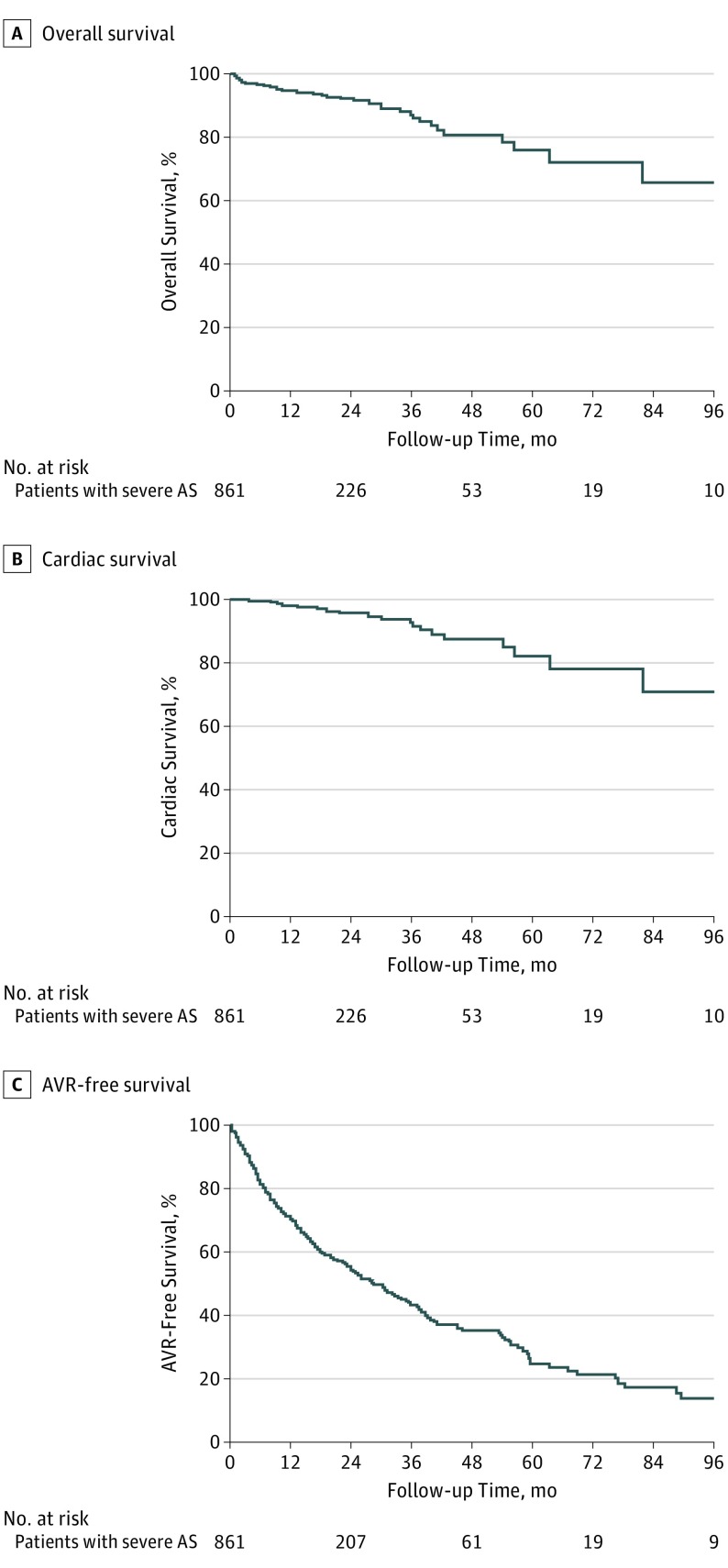
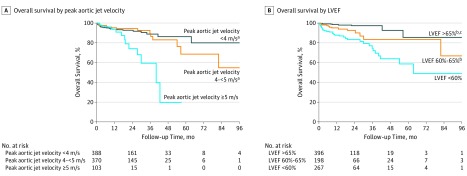
Results: Of the 1375 patients included in this analysis, 834 (60.7%) were male, and the mean (SD) age was 71 (13) years. A total of 861 patients (62.6%) had severe AS (aortic valve area less than 1.0 cm2). The mean (SD) overall survival during medical management (mean [SD] follow up, 27 [24] months) was 93% (1%), 86% (2%), and 75% (4%) at 2, 4, and 8 years, respectively. A total of 104 patients (7.6%) died under observation, including 57 patients (54.8%) from cardiovascular causes. The crude rate of sudden death was 0.65% over the duration of the study. A total of 542 patients (39.4%) underwent AVR, including 388 patients (71.6%) with severe AS at study entry and 154 (28.4%) with moderate AS at entry who progressed to severe AS. Those with severe AS at entry who underwent AVR did so at a mean (SD) of 14.4 (16.6) months and a median of 8.7 months. The mean (SD) 2-year and 4-year AVR-free survival rates for asymptomatic patients with severe AS at baseline were 54% (2%) and 32% (3%), respectively. In those undergoing AVR, the 30-day postprocedural mortality was 0.9%. In patients with severe AS at entry, peak aortic jet velocity (greater than 5 m/s) and LVEF (less than 60%) were associated with all-cause and cardiovascular mortality without AVR; these factors were also associated with postprocedural mortality in those patients with severe AS at baseline who underwent AVR (surgical AVR in 310 patients; transcatheter AVR in 78 patients).
Conclusions and relevance: In patients with asymptomatic AS followed up in heart valve centers, the risk of sudden death is low, and rates of overall survival are similar to those reported from previous series. Patients with severe AS at baseline and peak aortic jet velocity of 5.0 m/s or greater or LVEF less than 60% have increased risks of all-cause and cardiovascular mortality even after AVR. The potential benefit of early intervention should be considered in these high-risk patients.
Conflict of interest statement
Figures
Comment in
-
Thresholds for Valve Replacement in Asymptomatic Patients With Aortic Stenosis.JAMA Cardiol. 2018 Nov 1;3(11):1068-1069. doi: 10.1001/jamacardio.2018.3277. JAMA Cardiol. 2018. PMID: 30285030 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
