

Effect of Early Surgery vs Physical Therapy on Knee Function Among Patients With Nonobstructive Meniscal Tears: The ESCAPE Randomized Clinical Trial
- PMID: 30285177
- PMCID: PMC6583004
- DOI: 10.1001/jama.2018.13308
Effect of Early Surgery vs Physical Therapy on Knee Function Among Patients With Nonobstructive Meniscal Tears: The ESCAPE Randomized Clinical Trial
Erratum in
-
Data Errors in Table 3.JAMA. 2018 Dec 4;320(21):2272-2273. doi: 10.1001/jama.2018.17900. JAMA. 2018. PMID: 30512083 Free PMC article. No abstract available.
-
Data Errors in Table 3 and Figure 1.JAMA. 2020 Mar 10;323(10):1001. doi: 10.1001/jama.2020.1316. JAMA. 2020. PMID: 32154847 Free PMC article. No abstract available.
Abstract
Importance: Despite recent studies suggesting arthroscopic partial meniscectomy (APM) is not more effective than physical therapy (PT), the procedure is still frequently performed in patients with meniscal tears.
Objective: To assess whether PT is noninferior to APM for improving patient-reported knee function in patients with meniscal tears.
Design, setting, and participants: Noninferiority, multicenter, randomized clinical trial conducted in 9 hospitals in the Netherlands. Participants were aged 45 to 70 years with nonobstructive meniscal tears (ie, no locking of the knee joint). Patients with knee instability, severe osteoarthritis, and body mass index greater than 35 were excluded. Recruitment took place between July 17, 2013, and November 4, 2015. Participants were followed up for 24 months (final participant follow-up, October 11, 2017).
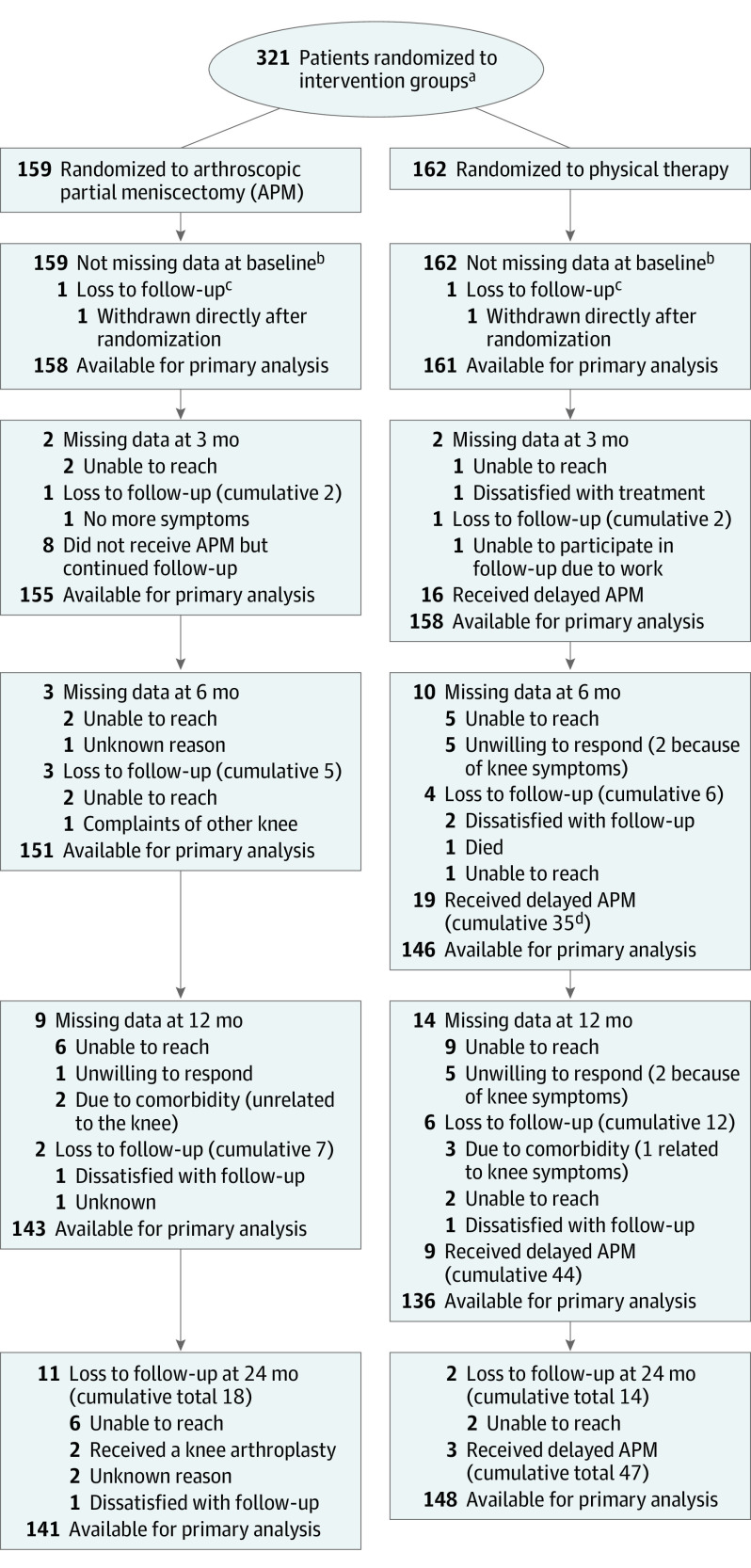
Interventions: Three hundred twenty-one participants were randomly assigned to APM (n = 159) or a predefined PT protocol (n = 162). The PT protocol consisted of 16 sessions of exercise therapy over 8 weeks focused on coordination and closed kinetic chain strength exercises.
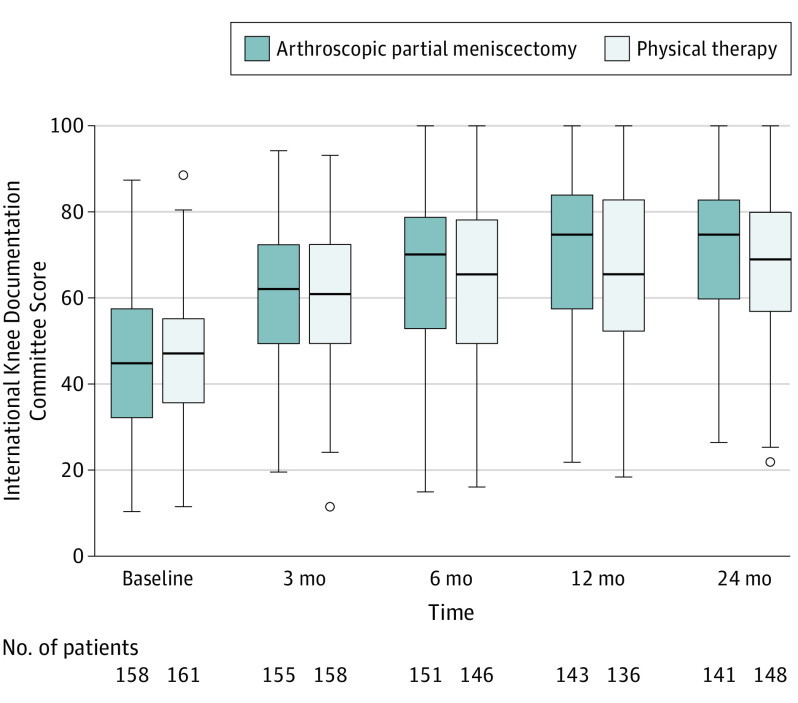
Main outcomes and measures: The primary outcome was change in patient-reported knee function on the International Knee Documentation Committee Subjective Knee Form (range, 0 to 100; from worse to best) from baseline over a 24-month follow-up period. The noninferiority margin was defined as a difference between treatment groups of 8 points and was assessed with a 1-sided α of .025. The primary analysis followed the intention-to-treat principle.
Results: Among 321 patients who were randomized (mean [SD] age, 58 [6.6] years; 161 women [50%]), 289 (90%) completed the trial (161 women and 158 men). In the PT group, 47 participants (29%) had APM during the 24-month follow-up period, and 8 participants randomized to APM (5%) did not have APM. Over a 24-month follow-up period, knee function improved in the APM group by 26.2 points (from 44.8 to 71.5) and in the PT group by 20.4 points (from 46.5 to 67.7). The overall between-group difference was 3.6 points (97.5% CI, -∞ to 6.5; P value for noninferiority = .001). Adverse events occurred in 18 participants in the APM group and 12 in the PT group. Repeat surgery (3 in the APM group and 1 in the PT group) and additional outpatient visits for knee pain (6 in the APM group and 2 in the PT group) were the most frequent adverse events.
Conclusions and relevance: Among patients with nonobstructive meniscal tears, PT was noninferior to APM for improving patient-reported knee function over a 24-month follow-up period. Based on these results, PT may be considered an alternative to surgery for patients with nonobstructive meniscal tears.
Trial registration: ClinicalTrials.gov Identifier: NCT01850719.
Conflict of interest statement
Figures
Comment in
-
Physical Therapy or Arthroscopic Surgery for Treatment of Meniscal Tears: Is Noninferiority Enough?JAMA. 2018 Oct 2;320(13):1326-1327. doi: 10.1001/jama.2018.13181. JAMA. 2018. PMID: 30285160 No abstract available.
-
Arthroscopic Partial Meniscectomy vs Physical Therapy for Nonobstructive Meniscal Tears.JAMA. 2019 Feb 26;321(8):805-806. doi: 10.1001/jama.2018.20261. JAMA. 2019. PMID: 30806685 No abstract available.
-
In Patients with Nonobstructive Meniscal Tears, Physiotherapy Was Noninferior to Arthroscopic Partial Meniscectomy for Knee Function Over a 24-Month Period.J Bone Joint Surg Am. 2019 May 15;101(10):941. doi: 10.2106/JBJS.19.00177. J Bone Joint Surg Am. 2019. PMID: 31094988 No abstract available.
-
Critically appraised paper: Physical therapy was noninferior to partial meniscectomy for improving knee function in patients with nonobstructive meniscal tears [synopsis].J Physiother. 2020 Oct;66(4):269. doi: 10.1016/j.jphys.2020.07.012. Epub 2020 Aug 23. J Physiother. 2020. PMID: 32847765 No abstract available.
-
Critically appraised paper: Physical therapy was noninferior to partial meniscectomy for improving knee function in patients with nonobstructive meniscal tears [commentary].J Physiother. 2020 Oct;66(4):269. doi: 10.1016/j.jphys.2020.08.002. Epub 2020 Sep 23. J Physiother. 2020. PMID: 32980311 No abstract available.
References
-
- Steiner CA, Karaca Z, Moore BJ, Imshaug MC, Pickens G. Surgeries in hospital-based ambulatory surgery and hospital inpatient settings, 2014. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb223-Ambulatory-Inpatien.... Accessed August 15, 2018. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
