

Trends in stroke outcomes in the last ten years in a European tertiary hospital
- PMID: 30285659
- PMCID: PMC6171303
- DOI: 10.1186/s12883-018-1164-7
Trends in stroke outcomes in the last ten years in a European tertiary hospital
Abstract
Background: Studying the impact of demographic changes and progress in the management of stroke patients is necessary in order to organize care structures for the coming years. Consequently, we analyzed the prognostic trends of patients admitted to the Stroke Unit of a tertiary hospital in the last ten years.
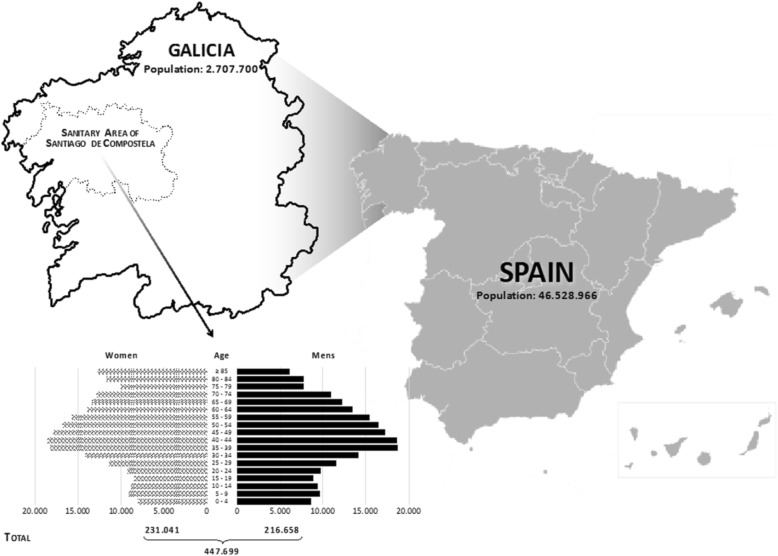
Methods: The University Clinical Hospital of Santiago de Compostela is the referral hospital for stroke in a catchment area that accounts for 16.5% of the population of Galicia. Data from patients admitted to the Stroke Unit were registered prospectively. A multinomial logistic regression was performed to determine the influence of new trends in demographic factors and in the management of patients with acute stroke. For the expected trend of progression, a 2008-2011 and 2012-2017 time series model was made by selecting the most appropriate model.
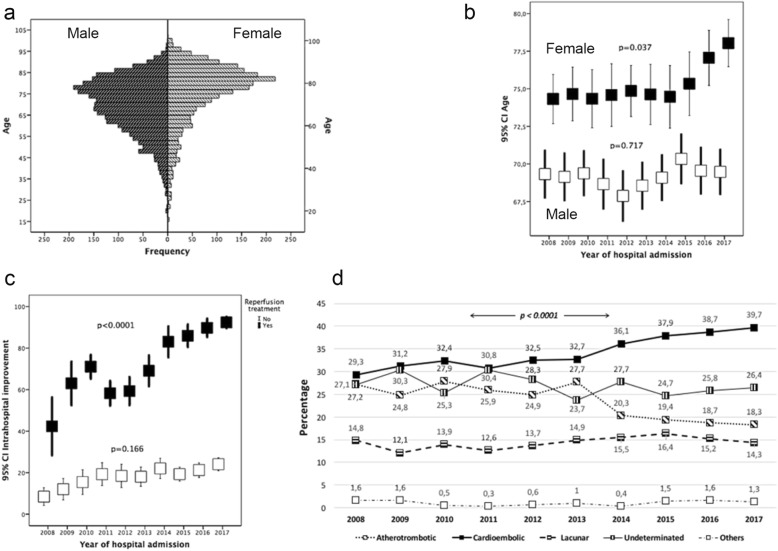
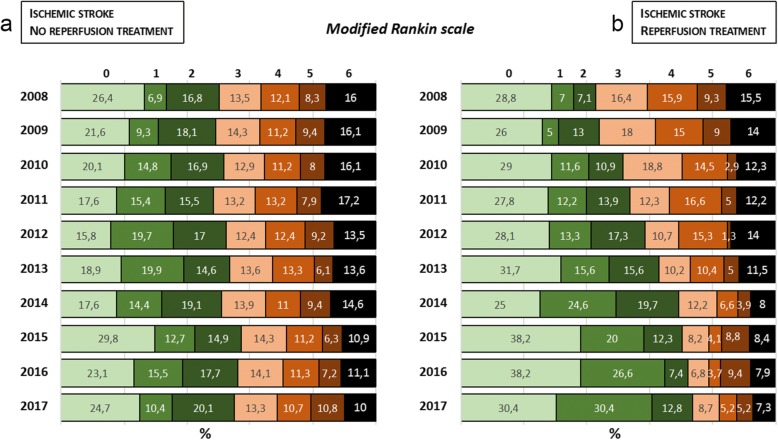
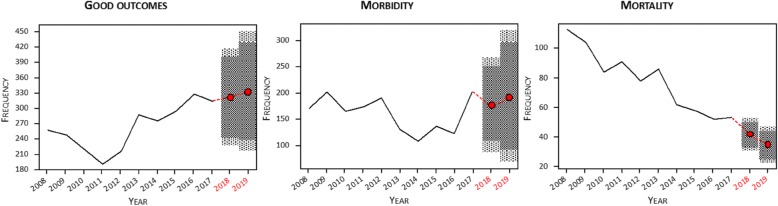
Results: In the last 10 years, the age of stroke onset has only increased in women (from 74.4 ± 2.2 years in 2008 to 78.8 ± 2.1 years in 2017; p = 0.037), and the same happens with the severity of neurological symptoms (ischemic stroke (IS), p < 0.0001; from 14 [10, 19] in 2008 to 19 [15, 26] in 2017), with a higher percentage of cardioembolic strokes (40.7% vs. 32.2% of cardioembolic strokes in women vs. men, p < 0.0001). In a multiple linear regression model, hospital improvement was mainly associated with the use of reperfusion treatment (B 53.11, CI 95% 49.87, 56.36, p < 0.0001). A differentiated multinomial logistic regression analysis conducted for the whole sample with ischemic strokes in the two time periods (2008-2011 and 2012-2017) showed no differences in the influence of factors associated with higher morbidity and mortality. The modeling of time series showed a distinct falling trend in mortality, with a slight increase in good outcome as well as morbidity in both ischemic and hemorrhagic stroke.
Conclusions: Our results showed that mortality decreased in the entire sample; however, although outcome at discharge improved in ischemic stroke, severe disability also increased in these patients. Importantly, this tendency towards increased morbidity seems to be confirmed for the coming years.
Keywords: Intracerebral hemorrhage; Ischemic stroke; Morbidity; Mortality.
Conflict of interest statement
Ethics approval and consent to participate
This research was conducted in accordance with the Declaration of Helsinki of the World Medical Association (2008) and approved by the Ethics Committee of Galicia (EC). Written informed consent was obtained from each patient after full discussion of the procedures. For patients who not being able to provide informed consent, their next of kin was contacted, discussed about study participation, and written informed consent was acquired.
Consent for publication
Not applicable.
Competing interests
The authors report no conflicts of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Demaerschalk BM, Kleindorfer DO, Adepye OM, Demchuck AM, Fugate JE, Grotta JC, et al. Scientific rationale for the inclusion and exclusion criteria for intravenous alteplase in acute ischemic stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47:581–641. doi: 10.1161/STR.0000000000000086. - DOI - PubMed
MeSH terms
Grants and funding
- SAF2014-56336-R and SAF2017-84267-R/Ministerio de Economía, Industria y Competitividad, Gobierno de España
- PI17/00540 and PI17/01103/Instituto de Salud Carlos III
- CPII17/00027/Instituto de Salud Carlos III
- CP14/00154/Instituto de Salud Carlos III
- RD16/0019/Spanish Research Network on Cerebrovascular Diseases RETICS-INVICTUS-PLUS
LinkOut - more resources
Full Text Sources
Medical
