

Prevalence and associated factors of pediatric emergency mortality at Tikur Anbessa specialized tertiary hospital: a 5 year retrospective case review study
- PMID: 30285667
- PMCID: PMC6167843
- DOI: 10.1186/s12887-018-1287-4
Prevalence and associated factors of pediatric emergency mortality at Tikur Anbessa specialized tertiary hospital: a 5 year retrospective case review study
Abstract
Background: Childhood mortality remains high in resource-limited third world countries. Most childhood deaths in hospital often occur within the first 24 h of admission. Many of these deaths are from preventable causes. This study aims to describe the patterns of mortality in children presenting to the pediatric emergency department.
Methods: This was a five-year chart review of deaths in pediatric patients aged 7 days to 13 years presenting to the Tikur Anbessa Specialized Tertiary Hospital (TASTH) from January 2012 to December 2016. Data were collected using a pretested, structured checklist, and analyzed using the SPSS Version 20. Multivariate analysis by logistic regression was carried out to estimate any measures of association between variables of interest and the primary outcome of death.
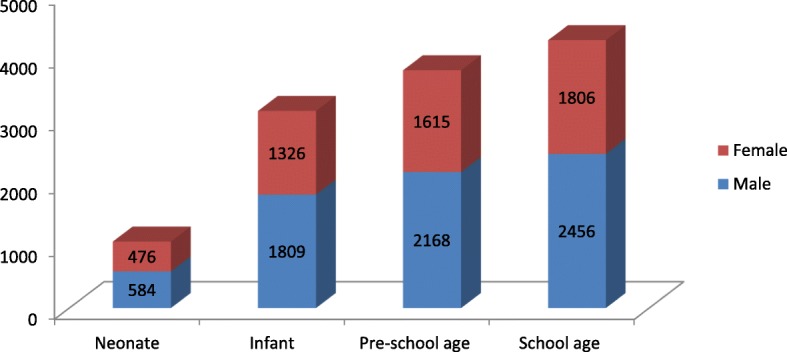
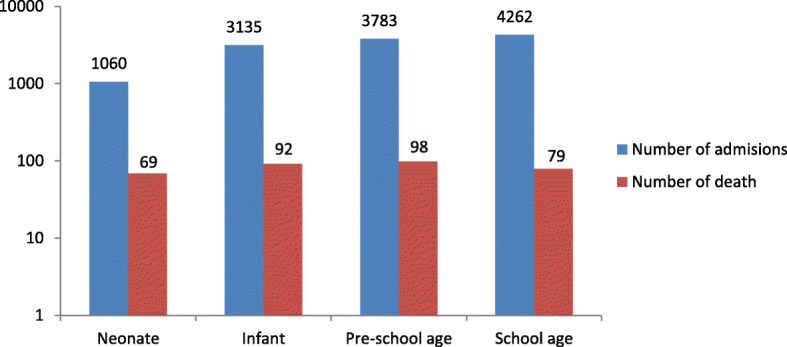
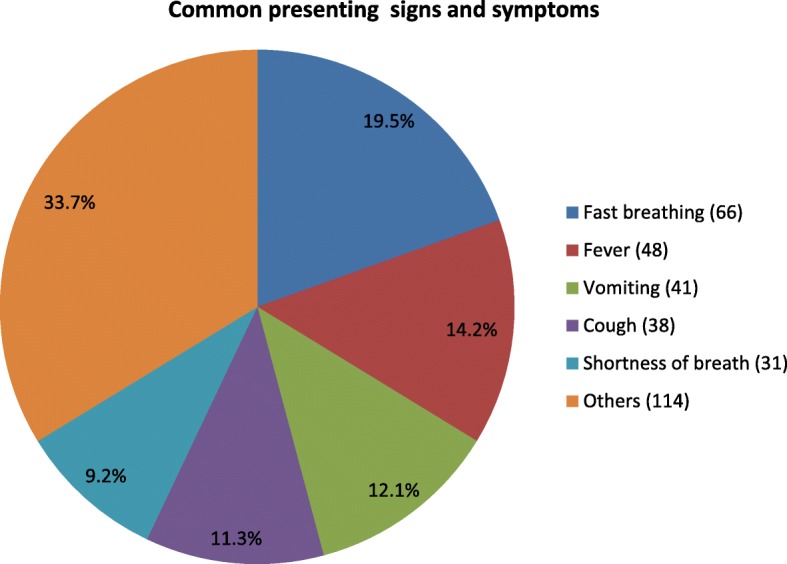
Results: The proportion of pediatric emergency department (PED) deaths was 4.1% (499 patients) out of 12,240 PED presentations. This translates to a mortality rate of 8.2 deaths per 1000 patients per year. The three top causes of deaths were pneumonia, congestive heart failure (CHF) and sepsis. Thirty two percent of the deaths occurred within 24 h of presentation with 6.5% of the deaths being neonates and the most common co-morbid illness was malnutrition (41.1%). Multivariate analysis revealed that shortness of breath [AOR=2.45, 95% CI (1.22-4.91)], late onset of signs and symptoms [AOR=3.22, 95% CI (1.34-7.73)], fever [AOR=3.17, 95% CI (1.28-7.86)], and diarrhea [AOR=3.36, 95% CI (1.69-6.67)] had significant association with early mortality.
Conclusion: The incidence of pediatric emergency mortality was high in our study. A delay in presentation of more than 48 hours, diarrheal diseases and shortness of breath were significantly associated with early pediatric mortality. Early identification and intervention are required to reduce pediatric emergency mortality.
Keywords: Emergency department; Ethiopia; Incidence; Pediatrics mortality.
Conflict of interest statement
Ethics approval and consent to participate
Ethical clearance and approval were obtained from the Ethical Committee of the Department of Emergency Medicine, College of Health Science, School of Medicine, Addis-Ababa University. Official letter was obtained from the Department of Emergency Medicine to the clinical director of TASTH. The ethical approval was received from the ethical committee for verbal consent from pediatric emergency department and Card Room staff before joining the study. Confidentiality was maintained in each level of the response. In view of the retrospective nature of this study and the secondary use of data from the health management information system database, study participant and family member consent was waived.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Rajaratnam JK, Marcus JR, Flaxman AD, Wang H, Levin-Rector A, Dwyer L, et al. Neonatal, postneonatal, childhood, and under-5 mortality for 187 countries, 1970–2010: a systematic analysis of progress towards millennium development goal 4. Lancet. 2010;375(9730):1988–2008. doi: 10.1016/S0140-6736(10)60703-9. - DOI - PubMed
-
- Organization WH . World health statistics 2010: World Health Organization. 2010.
-
- Harper Scott A., Bradley John S., Englund Janet A., File Thomas M., Gravenstein Stefan, Hayden Frederick G., McGeer Allison J., Neuzil Kathleen M., Pavia Andrew T., Tapper Michael L., Uyeki Timothy M., Zimmerman Richard K. Seasonal Influenza in Adults and Children—Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management: Clinical Practice Guidelines of the Infectious Diseases Society of America. Clinical Infectious Diseases. 2009;48(8):1003–1032. doi: 10.1086/598513. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
