

Impact of graft and tunnel orientation on patient-reported outcome in anterior cruciate ligament reconstruction using bone-patellar tendon-bone autografts
- PMID: 30285815
- PMCID: PMC6171132
- DOI: 10.1186/s13018-018-0954-3
Impact of graft and tunnel orientation on patient-reported outcome in anterior cruciate ligament reconstruction using bone-patellar tendon-bone autografts
Abstract
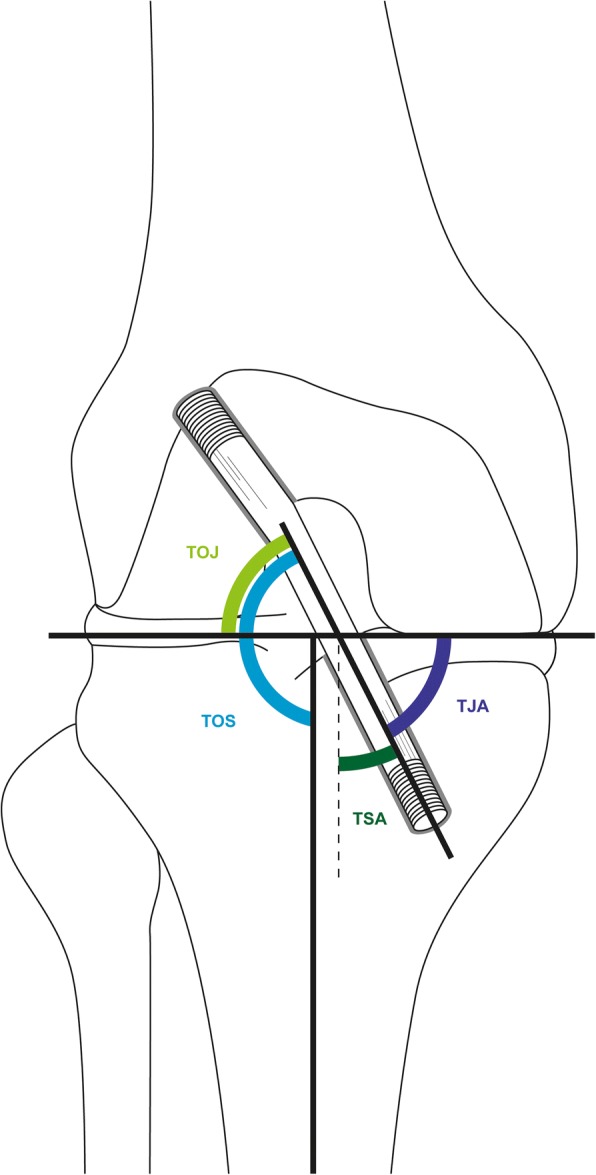
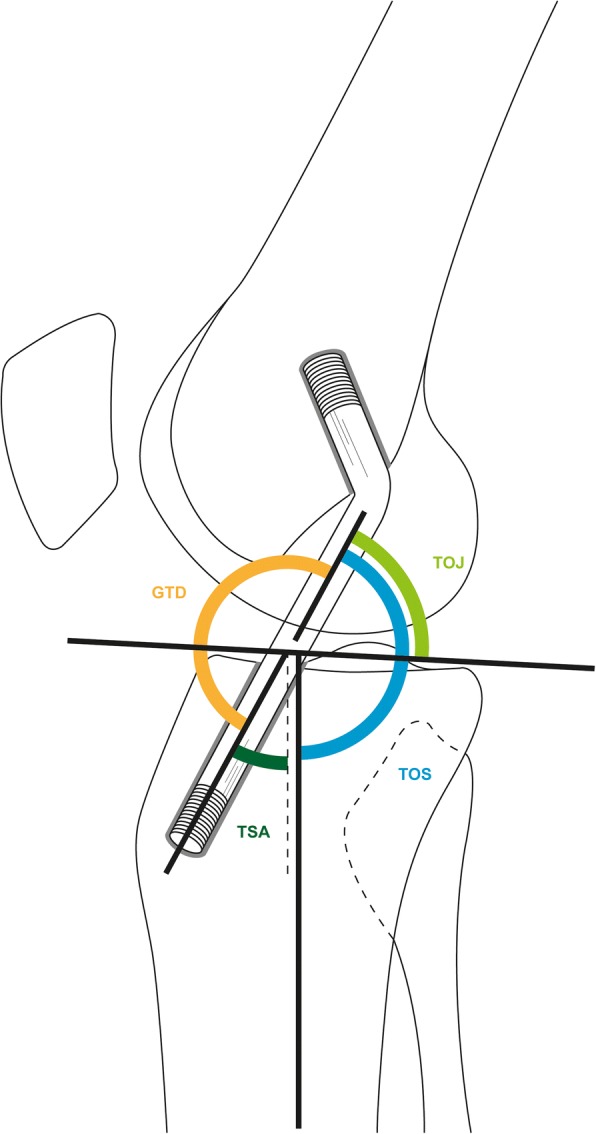
Background: The optimal positioning of anterior cruciate ligament graft is still controversially discussed. We therefore wanted to determine the tunnel-to-joint (TJA), tunnel-to-shaft (TSA), and graft-tunnel divergence angles which would provide the best outcome, determined by the KOOS (Knee Injury and Osteoarthritis Outcome Score). This study evaluated the clinical influence of graft orientation as measured with the KOOS questionnaire in patients with anterior cruciate ligament reconstruction with bone-patellar tendon-bone autografts.
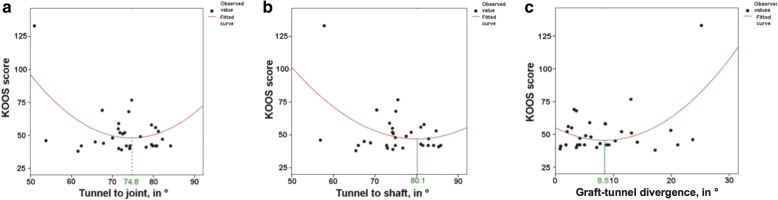
Methods: We designed a prospective cohort study, with a 1 ¼ year recruitment phase from March 2011 to July 2012 and a minimal follow-up period of 1 year. Inclusion criteria were patients ≥ 18 years of age receiving an ACL reconstruction with bone-patellar tendon-bone autografts at our institution after having suffered an acute ACL rupture. The primary outcome was the KOOS. Independent variables were patient age, gender, laterality of rupture, mechanism of trauma, and type of femoral and tibial fixation, as well as sagittal graft-tunnel divergence, TJA, and TSA, the latter two being assessed on coronal slices of magnetic resonance imaging. Equations modeling the relationship between TJA, TSA, and graft-tunnel divergence with the KOOS overall score were fitted, and the optimum angles were mathematically determined.
Results: In total, 31 patients were included in our study. Our cohort with a median age of 28 years was predominantly male. The mathematically determined optimal placement of the implant in the coronal plane was a TJA of 74.8°, a TSA of 80.1°, and a graft-tunnel divergence angle of 8.5°.
Conclusion: With regard to patient-reported outcome, the optimal graft orientation is provided by a coronal tunnel-to-shaft angle of 80° and tunnel-to-joint angle of 75°, respectively. Interestingly, in our series, patients reported best clinical outcomes with a sagittal graft-tunnel divergence. These results should be validated in larger studies.
Keywords: ACL reconstruction; Anterior cruciate ligament; Bone-patellar tendon-bone; Graft orientation; Outcome.
Conflict of interest statement
Ethics approval and consent to participate
Patient consent was obtained from all patients prior to study inclusion. The study was approved by the Cantonal Ethics Committee Zurich (ref. 2010-0437).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Goebel J. C., Bolbos R., Pham M., Galois L., Rengle A., Loeuille D., Netter P., Gillet P., Beuf O., Watrin-Pinzano A. In vivo high-resolution MRI (7T) of femoro-tibial cartilage changes in the rat anterior cruciate ligament transection model of osteoarthritis: a cross-sectional study. Rheumatology. 2010;49(9):1654–1664. doi: 10.1093/rheumatology/keq154. - DOI - PubMed
-
- Jepsen CF, Lundberg-Jensen AK, Faunoe P. Does the position of the femoral tunnel affect the laxity or clinical outcome of the anterior cruciate ligament-reconstructed knee? A clinical, prospective, randomized, double-blind study. Arthroscopy. 2007;23:1326–1333. doi: 10.1016/j.arthro.2007.09.010. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
