

Toward population specific and personalized treatment of Helicobacter pylori infection
- PMID: 30285834
- PMCID: PMC6167866
- DOI: 10.1186/s12929-018-0471-z
Toward population specific and personalized treatment of Helicobacter pylori infection
Abstract
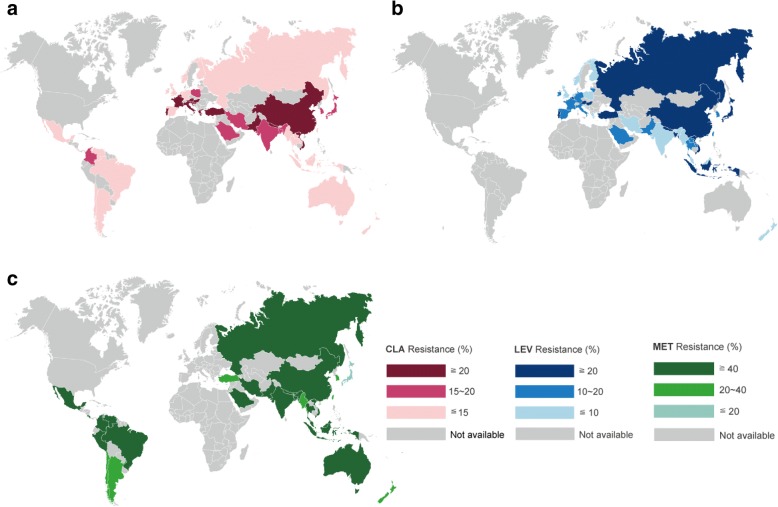
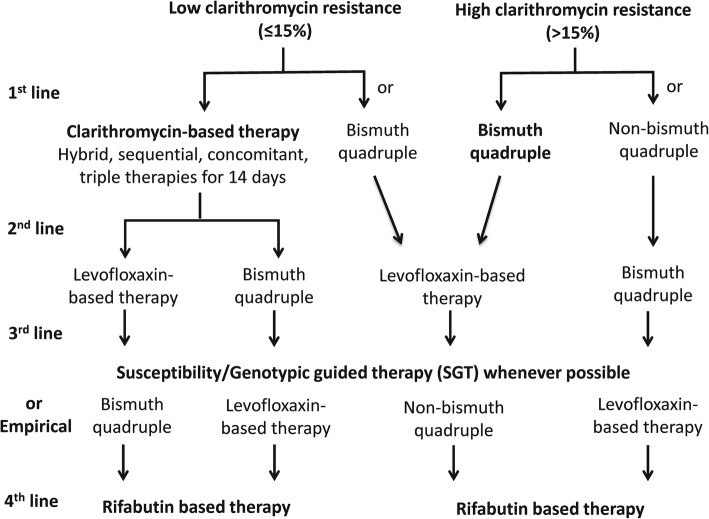
In the face of rising prevalence of antibiotic resistance, susceptibility testing to provide personalized treatment is recommended prior to eradication therapy for Helicobacter pylori (H. pylori). Yet, population specific treatment according to the local prevalence of antibiotic resistance may be an alternative if susceptibility testing is not available. In this article, we reviewed the global prevalence of primary antibiotic resistance and the efficacies of commonly used regimens in antibiotic susceptible and resistance strains. We then constructed a model to predict the efficacies of these regimens and proposed an algorithm to choose the optimal first-line and rescue therapies according to the prevalence of antibiotic resistance. Clarithromycin-based therapy (triple, sequential, concomitant, and hybrid therapies) for 14 days remains the treatment of choice in regions with low clarithromycin resistance (≤15%) and bismuth quadruple therapy may be an alternative therapy. In regions with high clarithromycin resistance (> 15%), bismuth quadruple therapy is the treatment of choice and non-bismuth quadruple therapy may be an alternative. Either levofloxacin-based therapy or bismuth quadruple therapy may be used as second-line rescue therapy for patients fail after clarithromycin-based therapies, whereas levofloxacin-based therapy may be used for patients fail after bismuth quadruple therapy. Susceptibility testing or genotypic resistance should be determined after two or more eradication failures. However, empirical therapy according to prior medication history to avoid the empirical reuse of levofloxacin and clarithromycin may be an acceptable alternative after consideration of cost, patient preference, and accessibility. Rifabutin-based therapy for 14 days may serve as the fourth-line therapy. New antibiotics specific for H. pylori are highly anticipated.
Keywords: Eradication; First-line; Gastric cancer; H. pylori; Precision medicine; Rescue; Resistance.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Lee Yi-Chia, Chiang Tsung-Hsien, Chou Chu-Kuang, Tu Yu-Kang, Liao Wei-Chih, Wu Ming-Shiang, Graham David Y. Association Between Helicobacter pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-analysis. Gastroenterology. 2016;150(5):1113-1124.e5. doi: 10.1053/j.gastro.2016.01.028. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
