

Assessment of left ventricular systolic and diastolic abnormalities in patients with hypertrophic cardiomyopathy using real-time three-dimensional echocardiography and two-dimensional speckle tracking imaging
- PMID: 30285887
- PMCID: PMC6167824
- DOI: 10.1186/s12947-018-0142-y
Assessment of left ventricular systolic and diastolic abnormalities in patients with hypertrophic cardiomyopathy using real-time three-dimensional echocardiography and two-dimensional speckle tracking imaging
Abstract
Background: Conventional echocardiography is not sensitive enough to assess left ventricular (LV) dysfunction in hypertrophic cardiomyopathy (HCM) patients. This research attempts to find a new ultrasonic technology to better assess LV diastolic function, systolic function, and myocardial longitudinal and circumferential systolic strain of segments with different thicknesses in HCM patients.
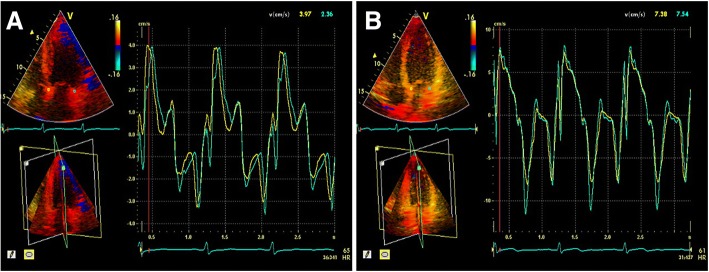
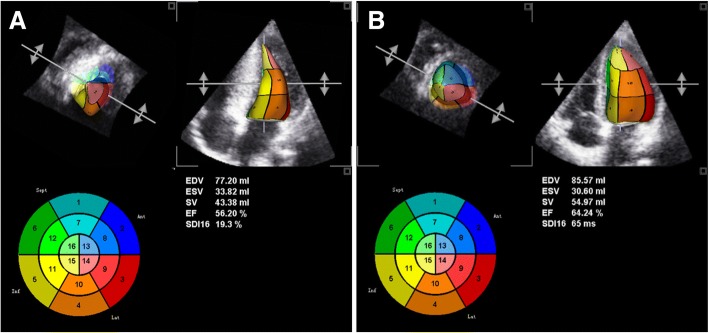
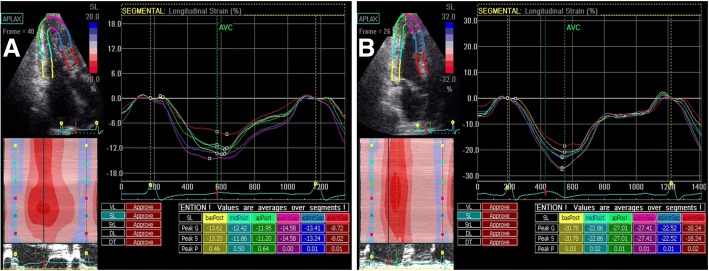
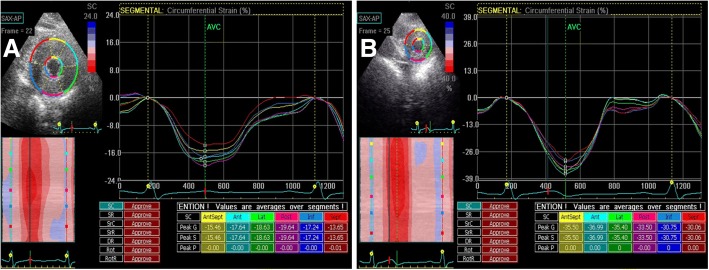
Methods: This study included 50 patients with HCM and 40 healthy subjects as controls. The peak early and late mitral annulus diastolic velocities at six loci (Ea' and Aa', respectively) and the Ea'/Aa' ratio were measured using real-time tri-plane echocardiography and quantitative tissue velocity imaging (RT-3PE-QTVI). The mean value of Ea' at six loci (Em') was obtained for the calculation of E/Em' ratio. The LV end-diastolic volume (LVEDV), LV end-systolic volume (LVESV), LV stroke volume (LVSV), and LV ejection fraction (LVEF) were measured using real-time three-dimensional echocardiography (RT-3DE). LV myocardial longitudinal peak systolic strain (LPSS) and circumferential peak systolic strain (CPSS) in the apical-middle-basal segments (LPSS-api, LPSS-mid, LPSS-bas; CPSS-api, CPSS-mid, and CPSS-bas, respectively) were obtained using a software for two-dimensional speckle tracking imaging (2D-STI). According to the different segmental thicknesses (STs) in each HCM patient, the values (LPSS and CPSS) of all the myocardial segments were categorized into three groups and the respective averages were computed.
Results: The Ea', Aa', and, Ea'/Aa' ratio in HCM patients were lower than those in the controls (all p < 0.001), while the E/Em' ratio in HCM patients was higher than that in the controls (p < 0.001). The LVEDV, LVSV, and LVEF were significantly lower in HCM patients than in controls (all p < 0.001). In HCM patients, the LPSS-api, LPSS-mid, LPSS-bas, CPSS-api, CPSS-mid, and CPSS-bas and the LPSS and CPSS of LV segments with different thicknesses were all significantly reduced (all p < 0.001).
Conclusions: In HCM patients, myocardial dysfunction was widespread not only in the obviously hypertrophic segments but also in the non-hypertrophic segments; the LV systolic and diastolic functions were damaged, even with a normal LVEF. LV diastolic dysfunction, systolic dysfunction, and myocardial deformation impairment in HCM patients can be sensitively revealed by RT-3PE-QTVI, RT-3DE, and 2D-STI.
Keywords: Diastolic functions; Hypertrophic cardiomyopathy; Left ventricular; Real-time three-dimensional; Real-time tri-plane echocardiography and quantitative tissue velocity imaging; Systolic functions; Two-dimensional speckle tracking imaging.
Conflict of interest statement
Ethics approval and consent to participate
This study has been approved by the Chinese PLA General Hospital Medical Ethics Committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All persons gave their informed consent prior to their inclusion in the study.
Consent for publication
All the authors contributed substantially to the project and agreed for sending the manuscript to
Competing interests
The authors declare that they have no conflict of interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
