

Adoptive transfer of tumor-infiltrating lymphocytes in melanoma: a viable treatment option
- PMID: 30285902
- PMCID: PMC6171186
- DOI: 10.1186/s40425-018-0391-1
Adoptive transfer of tumor-infiltrating lymphocytes in melanoma: a viable treatment option
Abstract
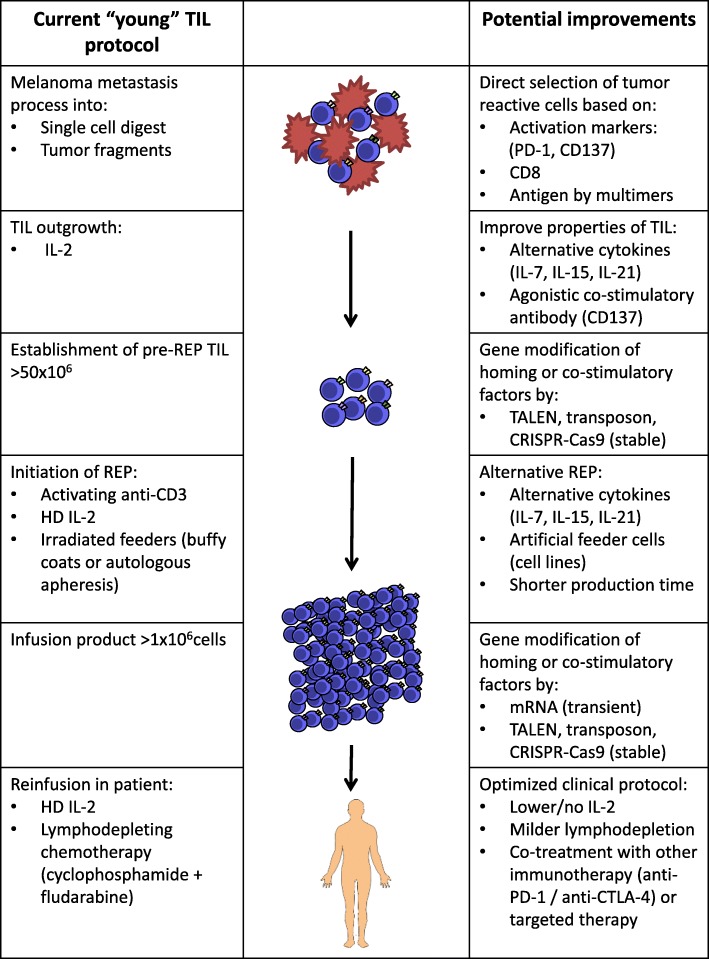
The treatment of metastatic melanoma patients with autologous tumor-infiltrating lymphocytes (TIL) shows robust, reproducible, clinical responses in clinical trials executed in several specialized centers over the world. Even in the era of targeted therapy and immune checkpoint inhibition, TIL therapy can be an additional and clinically relevant treatment line. This review provides an overview of the clinical experiences with TIL therapy thus far, including lymphodepleting regimens, the use of interleukin-2 (IL-2) and the associated toxicity. Characteristics of the TIL products and the antigen recognition pattern will be discussed, as well as the current and upcoming production strategies, including the selective expansion of specific fractions from the cell product. In addition, the future potential of TIL therapy in melanoma and other tumor types will be covered.
Keywords: Adoptive cell therapy; Antigen recognition; Combination therapy; Immunotherapy; Interleukin-2; Lymphodepletion; Melanoma; Tumor-infiltrating lymphocytes.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
MR declares to have no competing interests. JB has received grants from NEON therapeutics, BMS and Medimmune. PK has received compensation for advisory roles from NEON therapeutics and Personalis and has received grants from Merck and BMS. Through JH, NKI has received compensation for advisory roles from BMS, Merck, Roche, NEON therapeutics, Pfizer and Ipsen and NKI has received grants from BMS, Merck, Novartis and NEON therapeutics.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources