

Factors Contributing to Congenital Syphilis Cases - New York City, 2010-2016
- PMID: 30286056
- PMCID: PMC6171893
- DOI: 10.15585/mmwr.mm6739a3
Factors Contributing to Congenital Syphilis Cases - New York City, 2010-2016
Abstract
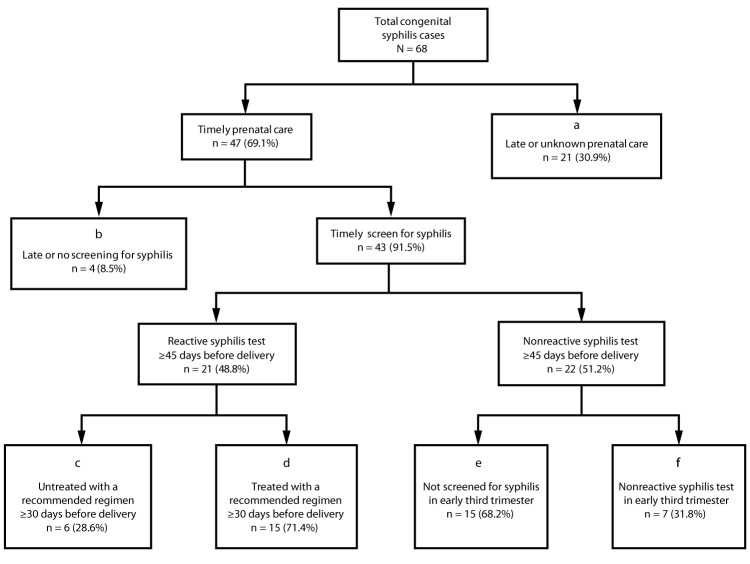
Congenital syphilis occurs when syphilis is transmitted from a pregnant woman to her fetus; congenital syphilis can be prevented through screening and treatment during pregnancy. Transmission to the fetus can occur at any stage of maternal infection, but is more likely during primary and secondary syphilis, with rates of transmission up to 100% at these stages (1). Untreated syphilis during pregnancy can cause spontaneous abortion, stillbirth, and early infant death. During 2013-2017, national rates of congenital syphilis increased from 9.2 to 23.3 cases per 100,000 live births (2), coinciding with increasing rates of primary and secondary syphilis among women of reproductive age (3). In New York City (NYC), cases of primary and secondary syphilis among women aged 15-44 years increased 147% during 2015-2016. To evaluate measures to prevent congenital syphilis, the NYC Department of Health and Mental Hygiene (DOHMH) reviewed data for congenital syphilis cases reported during 2010-2016 and identified patient-, provider-, and systems-level factors that contributed to these cases. During this period, 578 syphilis cases among pregnant women aged 15-44 years were reported to DOHMH; a congenital syphilis case was averted or otherwise failed to occur in 510 (88.2%) of these pregnancies, and in 68, a case of congenital syphilis occurred (eight cases per 100,000 live births).* Among the 68 pregnant women associated with these congenital syphilis cases, 21 (30.9%) did not receive timely (≥45 days before delivery) prenatal care. Among the 47 pregnant women who did access timely prenatal care, four (8.5%) did not receive an initial syphilis test until <45 days before delivery, and 22 (46.8%) acquired syphilis after an initial nonreactive syphilis test. These findings support recommendations that health care providers screen all pregnant women for syphilis at the first prenatal care visit and then rescreen women at risk in the early third trimester.
Conflict of interest statement
All authors have completed and submitted the ICMJE form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- American Academy of Pediatrics. Red book: 2018–2021 report of the Committee on Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2012.
-
- CDC. Sexually transmitted disease surveillance 2017. Atlanta, GA: US Department of Health and Human Services, CDC; 2018. https://www.cdc.gov/std/stats
-
- Cord blood test for syphilis. New York codes, rules and regulations. Title 10, section 69-2.2; 1989. https://regs.health.ny.gov/content/section-69-22-cord-blood-test-syphilis
MeSH terms
LinkOut - more resources
Full Text Sources
