

Results of a multicentre randomised controlled trial of cochlear-sparing intensity-modulated radiotherapy versus conventional radiotherapy in patients with parotid cancer (COSTAR; CRUK/08/004)
- PMID: 30286418
- PMCID: PMC6202674
- DOI: 10.1016/j.ejca.2018.08.006
Results of a multicentre randomised controlled trial of cochlear-sparing intensity-modulated radiotherapy versus conventional radiotherapy in patients with parotid cancer (COSTAR; CRUK/08/004)
Abstract
Purpose: About 40-60% of patients treated with post-operative radiotherapy for parotid cancer experience ipsilateral sensorineural hearing loss. Intensity-modulated radiotherapy (IMRT) can reduce radiation dose to the cochlea. COSTAR, a phase III trial, investigated the role of cochlear-sparing IMRT (CS-IMRT) in reducing hearing loss.
Methods: Patients (pT1-4 N0-3 M0) were randomly assigned (1:1) to 3-dimensional conformal radiotherapy (3DCRT) or CS-IMRT by minimisation, balancing for centre and radiation dose of 60Gy or 65Gy in 30 daily fractions. The primary end-point was proportion of patients with sensorineural hearing loss in the ipsilateral cochlea of ≥10 dB bone conduction at 4000 Hz 12 months after radiotherapy compared using Fisher's exact test. Secondary end-points included hearing loss at 6 and 24 months, balance assessment, acute and late toxicity, patient-reported quality of life, time to recurrence and survival.
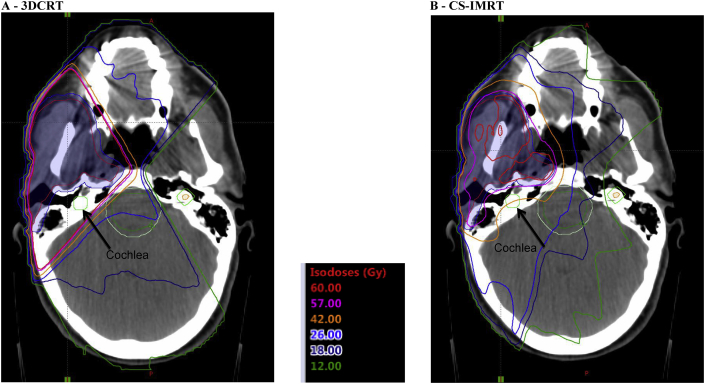
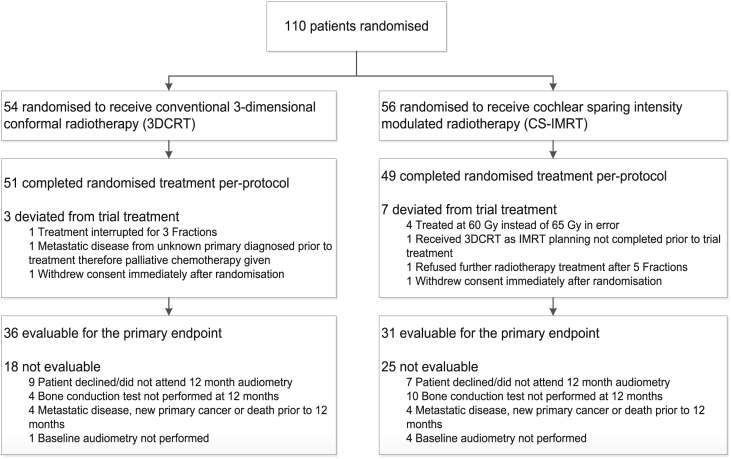
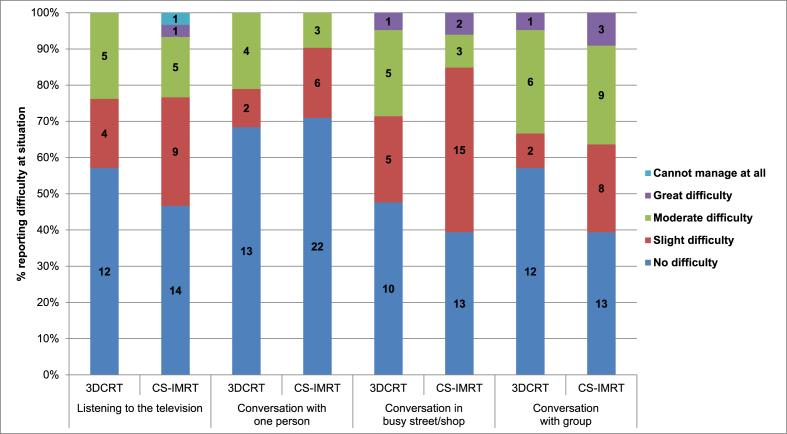
Results: From Aug 2008 to Feb 2013, 110 patients (54 3DCRT; 56 CS-IMRT) were enrolled from 22 UK centres. Median doses to the ipsilateral cochlea were 3DCRT: 56.2Gy and CS-IMRT: 35.7Gy (p < 0.0001). 67/110 (61%) patients were evaluable for the primary end-point; main reasons for non-evaluability were non-attendance at follow-up or incomplete audiology assessment. At 12 months, 14/36 (39%) 3DCRT and 11/31 (36%) CS-IMRT patients had ≥10 dB loss (p = 0.81). No statistically significant differences were observed in hearing loss at 6 or 24 months or in other secondary end-points including patient-reported hearing outcomes.
Conclusion: CS-IMRT reduced the radiation dose below the accepted tolerance of the cochlea, but this did not lead to a reduction in the proportion of patients with clinically relevant hearing loss.
Keywords: Cochlear-sparing; Head and neck cancer; Hearing loss; IMRT; Radiotherapy.
Copyright © 2018 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Spiro R.H. Salivary neoplasms: overview of a 35-year experience with 2,807 patients. Head Neck Surg. 1986;8:177–184. - PubMed
-
- Fitzpatrick P.J., Theriault C. Malignant salivary gland tumors. Int J Radiat Oncol Biol Phys. 1986;12:1743–1747. - PubMed
-
- Matsuba H.M., Thawley S.E., Devineni V.R. High-grade malignancies of the parotid gland: effective use of planned combined surgery and irradiation. Laryngoscope. 1985;95:1059–1063. - PubMed
-
- North C.A., Lee D.J., Piantadosi S. Carcinoma of the major salivary glands treated by surgery or surgery plus postoperative radiotherapy. Int J Radiat Oncol Biol Phys. 1990;18:1319–1326. - PubMed
-
- Garden A.S., el-Naggar A.K., Morrison W.H. Postoperative radiotherapy for malignant tumors of the parotid gland. Int J Radiat Oncol Biol Phys. 1997;37:79–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
