

A simulation tool for better management of retinal services
- PMID: 30286750
- PMCID: PMC6172737
- DOI: 10.1186/s12913-018-3560-5
A simulation tool for better management of retinal services
Abstract
Background: Advances in the management of retinal diseases have been fast-paced as new treatments become available, resulting in increasing numbers of patients receiving treatment in hospital retinal services. These patients require frequent and long-term follow-up and repeated treatments, resulting in increased pressure on clinical workloads. Due to limited clinic capacity, many National Health Service (NHS) clinics are failing to maintain recommended follow-up intervals for patients receiving care. As such, clear and robust, long term retinal service models are required to assess and respond to the needs of local populations, both currently and in the future.
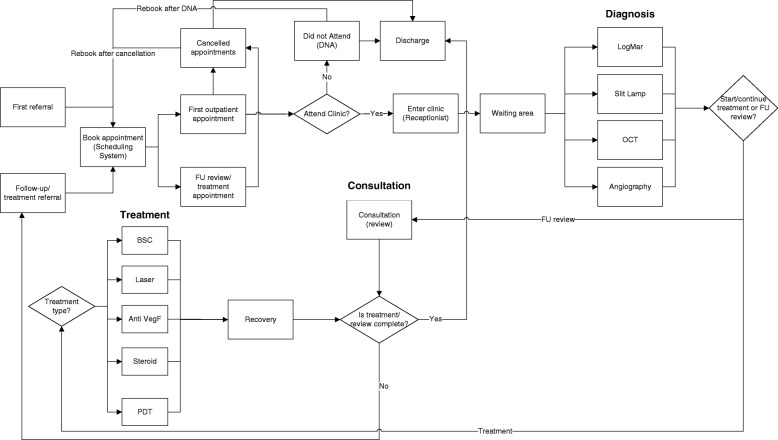
Methods: A discrete event simulation (DES) tool was developed to facilitate the improvement of retinal services by identifying efficiencies and cost savings within the pathway of care. For a mid-size hospital in England serving a population of over 500,000, we used 36 months of patient level data in conjunction with statistical forecasting and simulation to predict the impact of making changes within the service.
Results: A simulation of increased demand and a potential solution of the 'Treat and Extend' (T&E) regimen which is reported to result in better outcomes, in combination with virtual clinics which improve quality, effectiveness and productivity and thus increase capacity is presented. Without the virtual clinic, where T&E is implemented along with the current service, we notice a sharp increase in the number of follow-ups, number of Anti-VEGF injections, and utilisation of resources. In the case of combining T&E with virtual clinics, there is a negligible (almost 0%) impact on utilisation of resources.
Conclusions: Expansion of services to accommodate increasing number of patients seen and treated in retinal services is feasible with service re-organisation. It is inevitable that some form of initial investment is required to implement service expansion through T&E and virtual clinics. However, modelling with DES indicates that such investment is outweighed by cost reductions in the long term as more patients receive optimal treatment and retain vision with better outcomes. The model also shows that the service will experience an average of 10% increase in surplus capacity.
Keywords: Discrete event simulation; Patient flow modelling; Retinal services; Treat and extend; Virtual clinics.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval and participant consent was not necessary as this study involved the use of the national Hospital Episodes Statistics (HES) dataset. Details about HES can be obtained at
Consent for publication
Not applicable.
Competing interests
David Southern is an employee of Pathway Communications. No conflicting relationship exists for the other authors regarding this article.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- UK Vision Strategy 2013–18. 2013. https://www.visionuk.org.uk/refreshed-uk-vision-strategy-2013-18/. Accessed 14 Nov 2014.
-
- Holz FG, Amoaku W, Donate J, Guymer RH, Kellner U, Schlingemann RO, Weichselberger A, Staurenghi G, SUSTAIN Study Group Safety and efficacy of a flexible dosing regimen of ranibizumab in neovascular age-related macular degeneration: the SUSTAIN study. Ophthalmology. 2011;118:663–671. doi: 10.1016/j.ophtha.2010.12.019. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
