

Government resource contributions to the private-not-for-profit sector in Uganda: evolution, adaptations and implications for universal health coverage
- PMID: 30286757
- PMCID: PMC6172798
- DOI: 10.1186/s12939-018-0843-8
Government resource contributions to the private-not-for-profit sector in Uganda: evolution, adaptations and implications for universal health coverage
Abstract
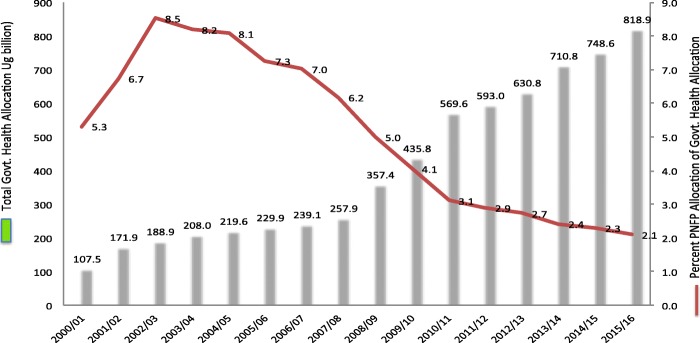
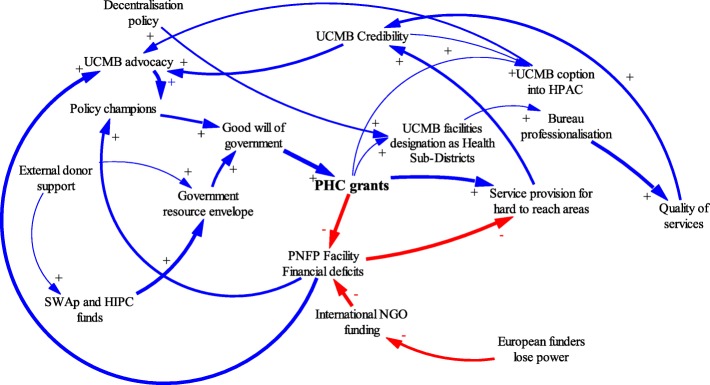
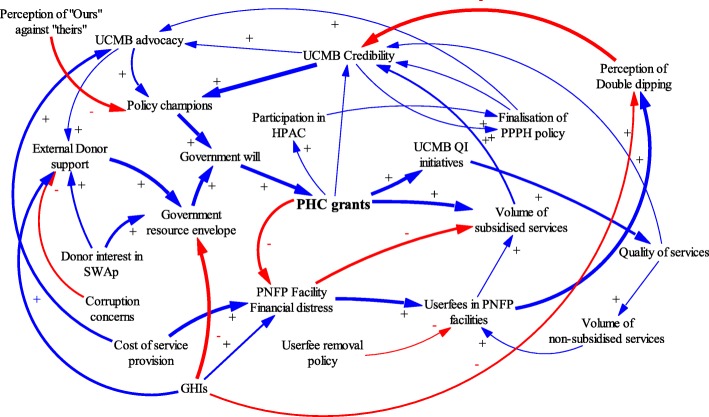
Background: A case study was prepared examining government resource contributions (GRCs) to private-not-for-profit (PNFP) providers in Uganda. It focuses on Primary Health Care (PHC) grants to the largest non-profit provider network, the Uganda Catholic Medical Bureau (UCMB), from 1997 to 2015. The framework of complex adaptive systems was used to explain changes in resource contributions and the relationship between the Government and UCMB.
Methods: Documents and key informant interviews with the important actors provided the main sources of qualitative data. Trends for GRCs and service outputs for the study period were constructed from existing databases used to monitor service inputs and outputs. The case study's findings were validated during two meetings with a broad set of stakeholders.
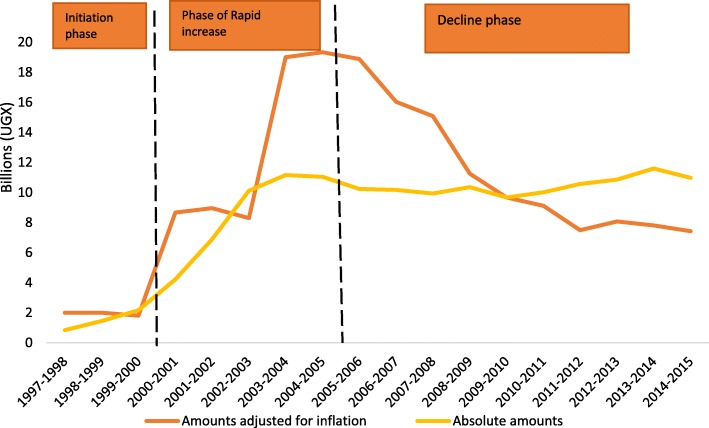
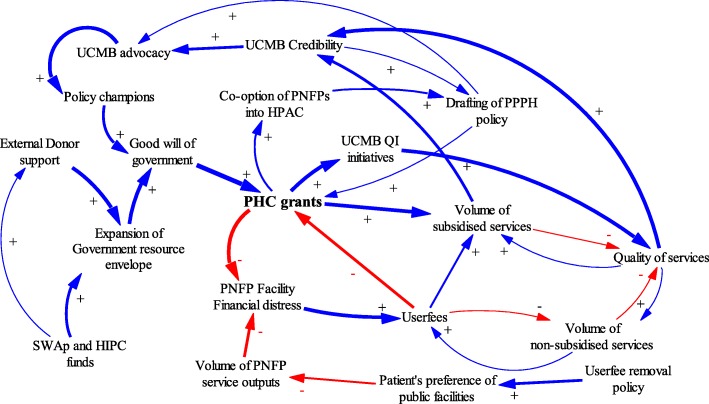
Results: Three major phases were identified in the evolution of GRCs and the relationship between the Government and UCMB: 1) Initiation, 2) Rapid increase in GRCs, and 3) Declining GRCs. The main factors affecting the relationship's evolution were: 1) Financial deficits at PNFP facilities, 2) advocacy by PNFP network leaders, 3) changes in the government financial resource envelope, 4) variations in the "good will" of government actors, and 5) changes in donor funding modalities. Responses to the above dynamics included changes in user fees, operational costs of PNFPs, and government expectations of UCMB. Quantitative findings showed a progressive increase in service outputs despite the declining value of GRCs during the study period.
Conclusions: GRCs in Uganda have evolved influenced by various factors and the complex interactions between government and PNFPs. The Universal Health Coverage (UHC) agenda should pay attention to these factors and their interactions when shaping how governments work with PNFPs to advance UHC. GRCs could be leveraged to mitigate the financial burden on communities served by PNFPs. Governments seeking to advance UHC goals should explore policies to expand GRCs and other modalities to subsidize the operational costs of PNFPs.
Keywords: Complex adaptive systems; Government subsidies; Non-state providers; Primary health care; Private-not-for-profit; Uganda; Universal health coverage.
Conflict of interest statement
Ethics approval and consent to participate
Approval was granted by Makerere University School of Public Health, Uganda National Council for Science and Technology and WHO Ethics Research Committee. Consent was sought and granted by all study participants.
Consent for publication
Not applicable.
Competing interests
AS, FS, JN, and SB declare that no competing interests. SO and RK are the senior managers of the Uganda Catholic Medical Bureau.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- World Health Assembly. Strengthening essential public health functions in support of the achievement of universal health coverage. Resolution WHA69.1; World Health Assembly, United Nations Geneva, Switzerland 2016.
-
- MOH . Systems H, 20/20;, School MU, Public. Uganda Health System Assessment 2011. Health systems 20/20 project, Abt associates Inc. 2012.
-
- MoH . National Health Policy II. 2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
