

Towards universal health coverage: a mixed-method study mapping the development of the faith-based non-profit sector in the Ghanaian health system
- PMID: 30286758
- PMCID: PMC6172851
- DOI: 10.1186/s12939-018-0810-4
Towards universal health coverage: a mixed-method study mapping the development of the faith-based non-profit sector in the Ghanaian health system
Abstract
Background: Faith-based non-profit (FBNP) providers have had a long-standing role as non-state, non-profit providers in the Ghanaian health system. They have historically been considered to be important in addressing the inequitable geographical distribution of health services and towards the achievement of universal health coverage (UHC), but in changing contexts, this contribution is being questioned. However, any assessment of contribution is hampered by the lack of basic information about their comparative presence and coverage in the Ghanaian health system. In response, since the 1950s, there have been repeated calls for the 'mapping' of faith-based health assets.
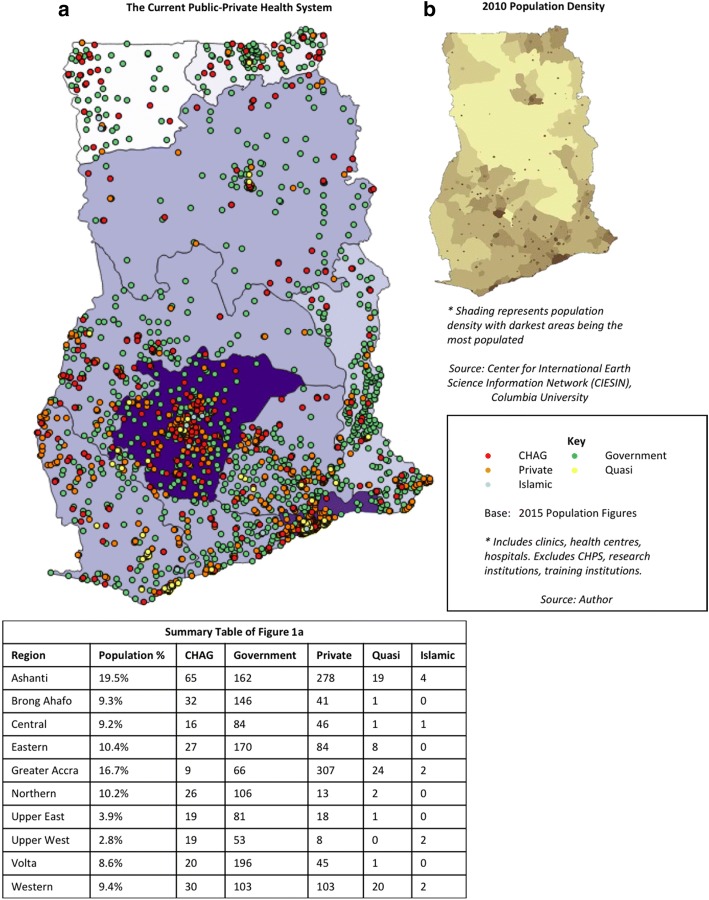
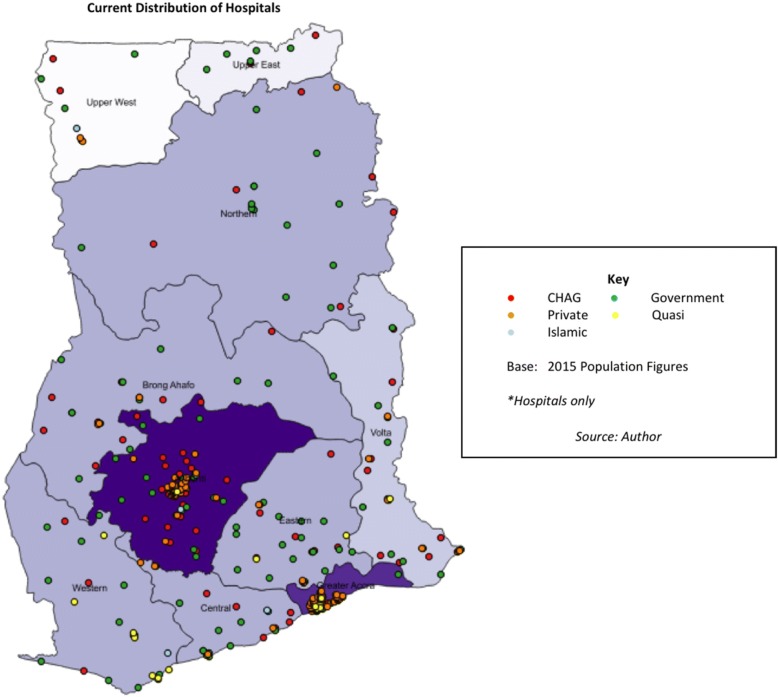
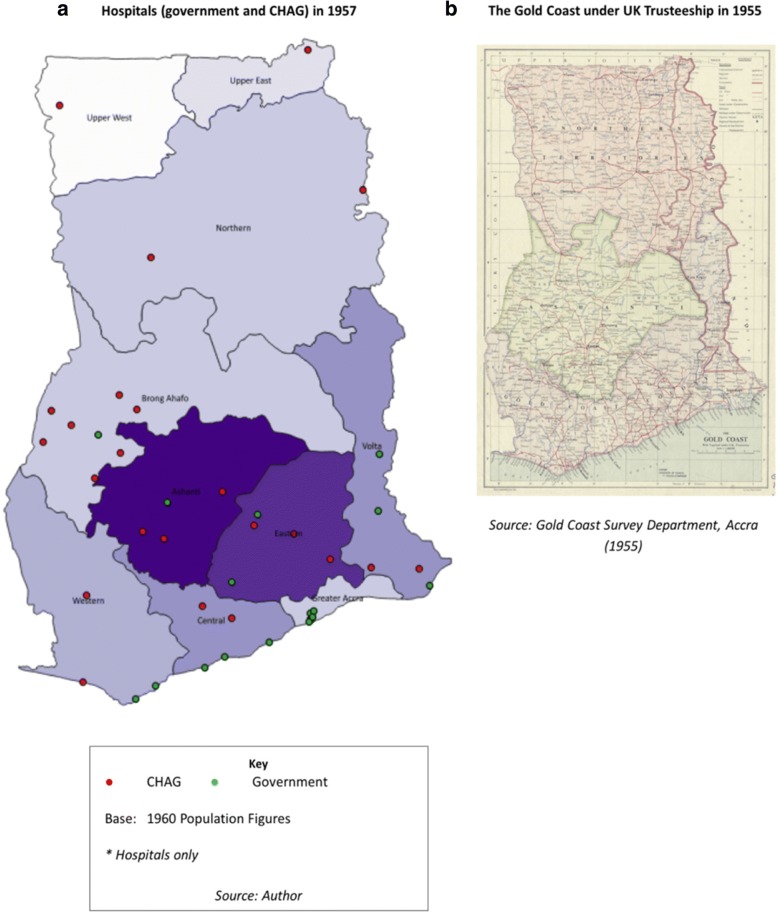
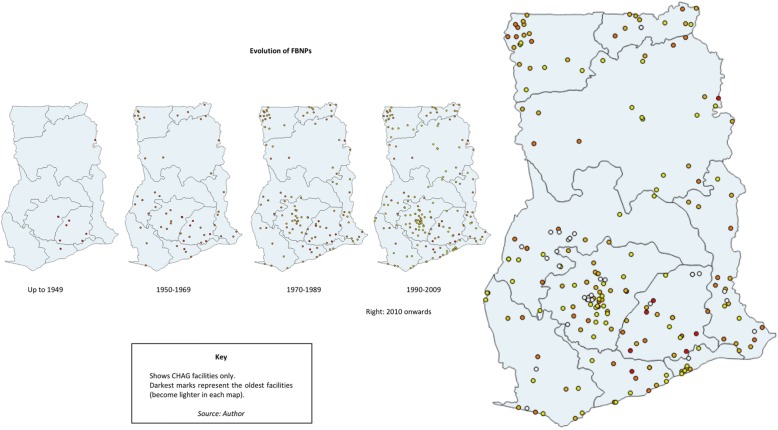
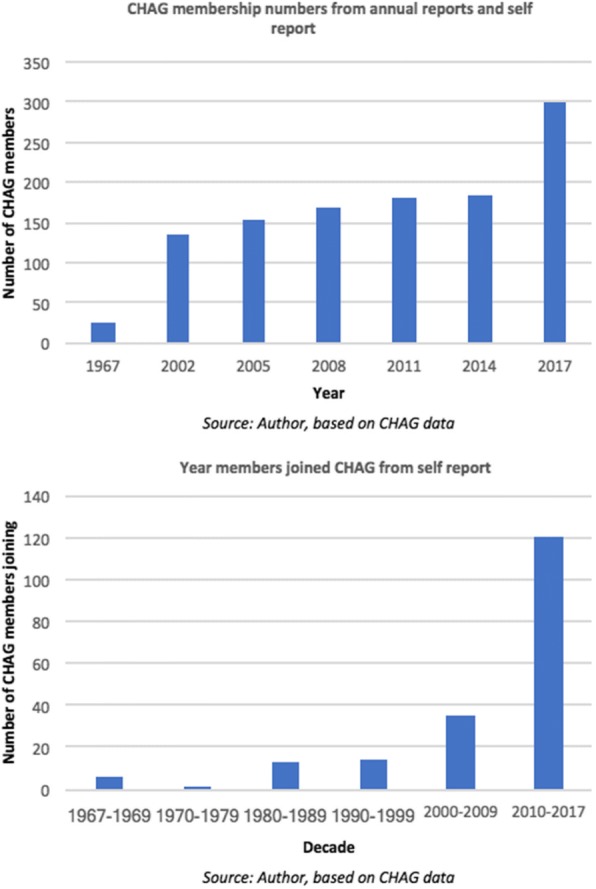
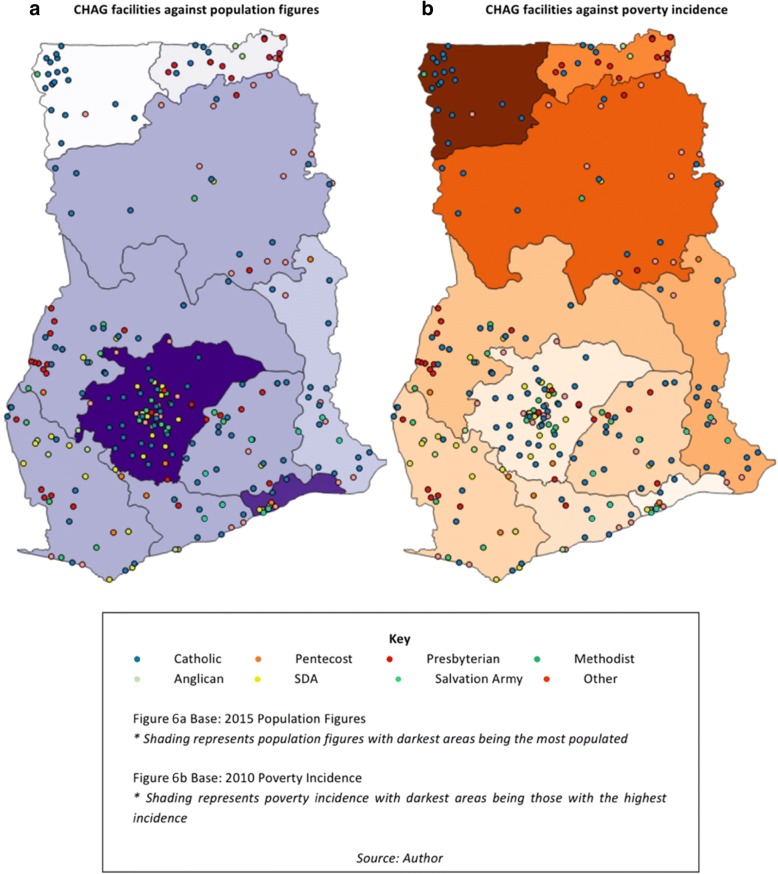
Methods: A historically-focused mixed-methods study was conducted, collecting qualitative and quantitative data and combining geospatial mapping with varied documentary resources (secondary and primary, current and archival). Geospatial maps were developed, providing a visual representation of changes in the spatial footprint of the Ghanaian FBNP health sector.
Results: The geospatial maps show that FBNPs were originally located in rural remote areas of the country but that this service footprint has evolved over time, in line with changing social, political and economic contexts.
Conclusion: FBNPs have had a long-standing role in the provision of health services and remain a valuable asset within national health systems in Ghana and sub-Saharan Africa more broadly. Collaboration between the public sector and such non-state providers, drawing on the comparative strengths and resources of FBNPs and focusing on whole system strengthening, is essential for the achievement of UHC.
Keywords: Faith-based providers; GIS; Ghana; Health system; History; Map; Non-state providers; Public-private partnership; Universal health coverage.
Conflict of interest statement
Authors’ information
Annabel Grieve is a post-graduate student at the University of Cape Town, School of Public Health and Family Medicine, Health Policy and Systems Division. This article was developed as part of a post-graduate dissertation project.
Jill Olivier is a Professor in the University of Cape Town, School of Public Health and Family Medicine, Health Policy and Systems Division. She is the co-PI of the larger study in Ghana (running from 2015 to 2018, funded by the AHPSR WHO), and was the thesis supervisor of the mapping sub-study.
Ethics approval and consent to participate
Although considered minimal risk, ethical approval was obtained from the University of Cape Town’s (UCT) Human Research Ethics Committee (HREC) (Reference 303/2017). The study also operated under the existing ethical considerations of the primary study, approval for which has been obtained from the WHO Research Ethics Committee, GHS Ethical Review Committee and UCT HREC (annually updated, 2015–2018).
Consent for publication
Yes, consent forms utilised in interviews – as part of larger primary study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organisation . Everybody’s business: strengthening health systems to improve health outcomes. WHO’s framework for action. Geneva: World Health Organisation; 2007.
-
- Gilson L. Health policy and systems research: a methodology reader. Geneva: Alliance for Health Policy and Systems Research, World Health Organisation; 2012.
-
- World Health Organisation . Service availability and readiness assessment (SARA): an annual monitoring system for service delivery. Reference manual, version 2.2 edition. Geneva: World Health Organisation; 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
