

The Changing Landscape of Diabetes Therapy for Cardiovascular Risk Reduction: JACC State-of-the-Art Review
- PMID: 30286929
- PMCID: PMC6178226
- DOI: 10.1016/j.jacc.2018.07.071
The Changing Landscape of Diabetes Therapy for Cardiovascular Risk Reduction: JACC State-of-the-Art Review
Abstract
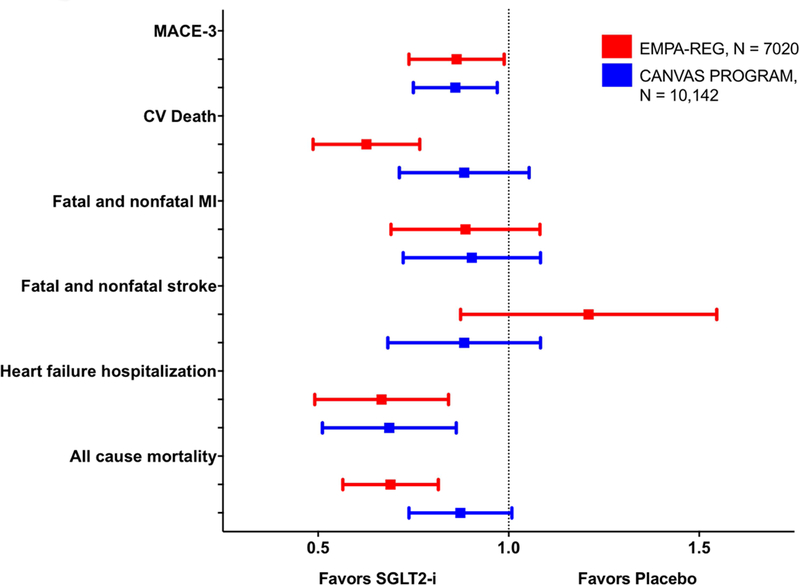
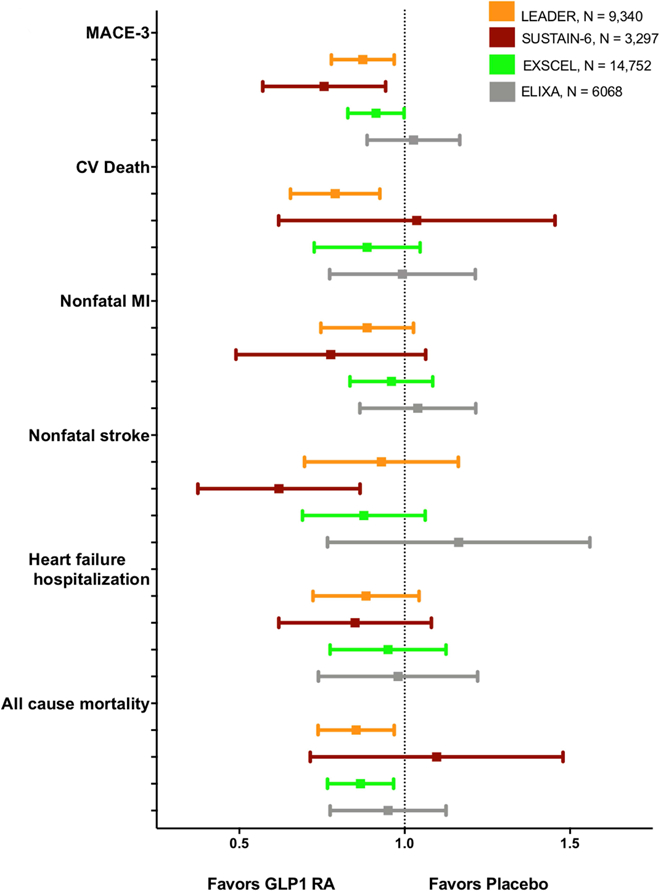
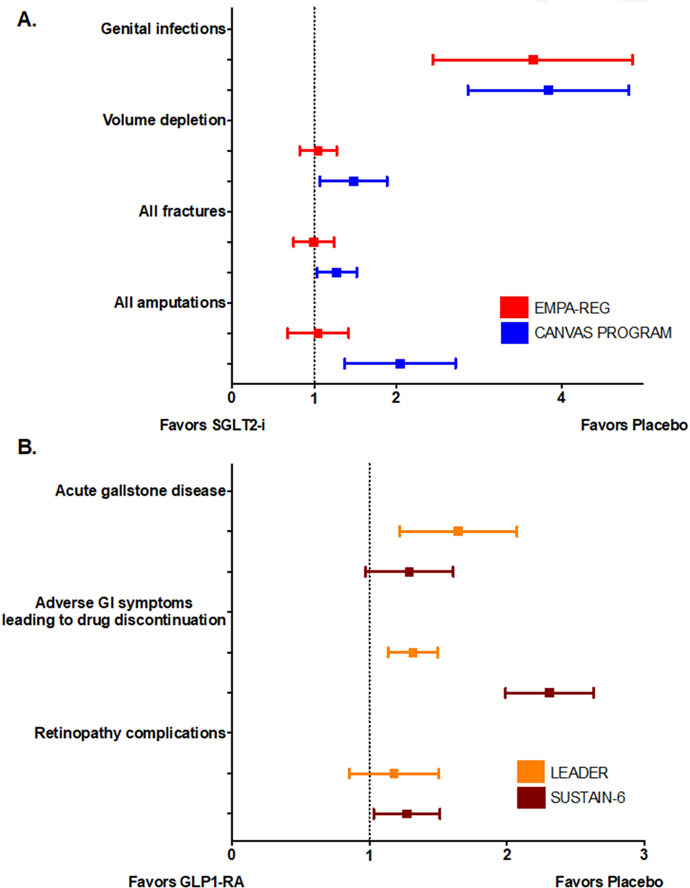
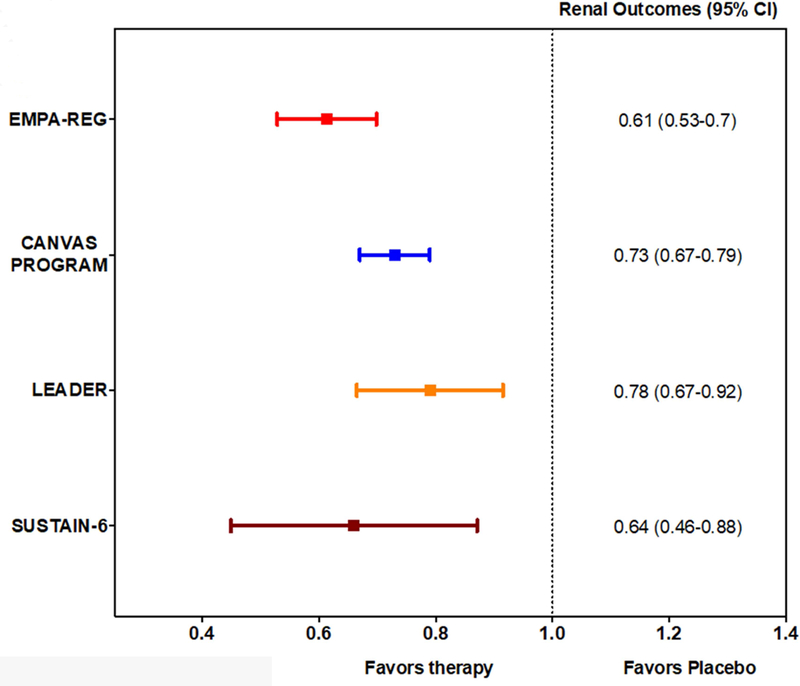
Type 2 diabetes mellitus (T2D) is a major risk factor for cardiovascular disease (CVD), the most common cause of death in T2D. Despite improved risk factor control, however, adults with T2D continue to experience substantial excess CVD risk. Until recently, however, improved glycemic control has not been associated with robust macrovascular benefit. The advent of 2 new classes of antihyperglycemic agents, the sodium-glucose cotransporter-2 inhibitors and the glucagon-like peptide-1 receptor agonists, and their respective large cardiovascular outcome trials, has led to a paradigm shift in how cardiologists and heath care practitioners conceptualize T2D treatment. Herein, the authors review the recent trial evidence, the potential mechanisms of action of the sodium-glucose cotransporter-2 inhibitors and the glucagon-like peptide-1 receptor agonists, safety concerns, and their use for the primary prevention of CVD as well as in diabetic patients with impaired renal function and heart failure.
Keywords: antidiabetic therapy; cardiovascular disease; primary prevention; secondary prevention; type 2 diabetes.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics−−2014 update: a report from the American Heart Association. Circulation 2014;129:e28–e292. Available at: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id.... - PMC - PubMed
-
- Gregg EW, Li Y, Wang J, et al. Changes in Diabetes-Related Complications in the United States, 1990–2010. N. Engl. J. Med 2014;370:1514–1523. - PubMed
-
- Ali MK, Bullard KM, Saaddine JB, Cowie CC, Imperatore G, Gregg EW. Achievement of goals in U.S. diabetes care, 1999–2010. N. Engl. J. Med 2013;368:1613–1624. - PubMed
-
- Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med 2015;373:2117–2128. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
