

Secondary findings from clinical genomic sequencing: prevalence, patient perspectives, family history assessment, and health-care costs from a multisite study
- PMID: 30287922
- PMCID: PMC6450774
- DOI: 10.1038/s41436-018-0308-x
Secondary findings from clinical genomic sequencing: prevalence, patient perspectives, family history assessment, and health-care costs from a multisite study
Erratum in
-
Correction: Secondary findings from clinical genomic sequencing: prevalence, patient perspectives, family history assessment, and health-care costs from a multisite study.Genet Med. 2019 May;21(5):1261-1262. doi: 10.1038/s41436-019-0440-2. Genet Med. 2019. PMID: 30670880
Abstract
Purpose: Clinical sequencing emerging in health care may result in secondary findings (SFs).
Methods: Seventy-four of 6240 (1.2%) participants who underwent genome or exome sequencing through the Clinical Sequencing Exploratory Research (CSER) Consortium received one or more SFs from the original American College of Medical Genetics and Genomics (ACMG) recommended 56 gene-condition pair list; we assessed clinical and psychosocial actions.
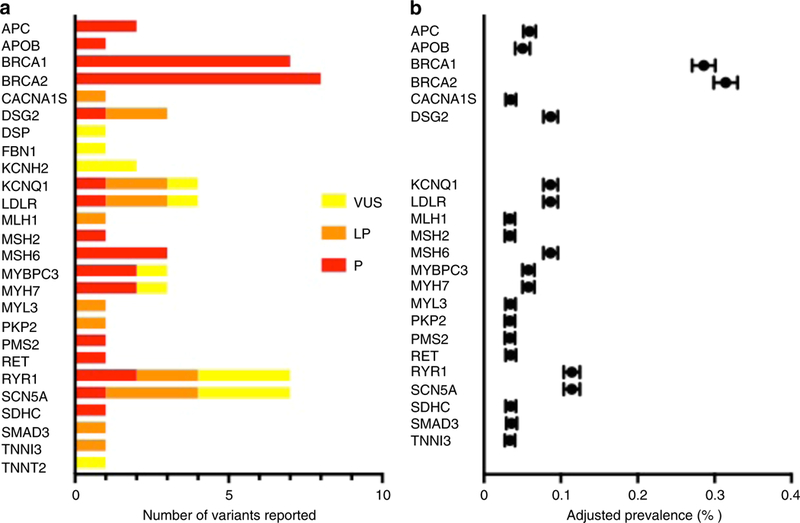
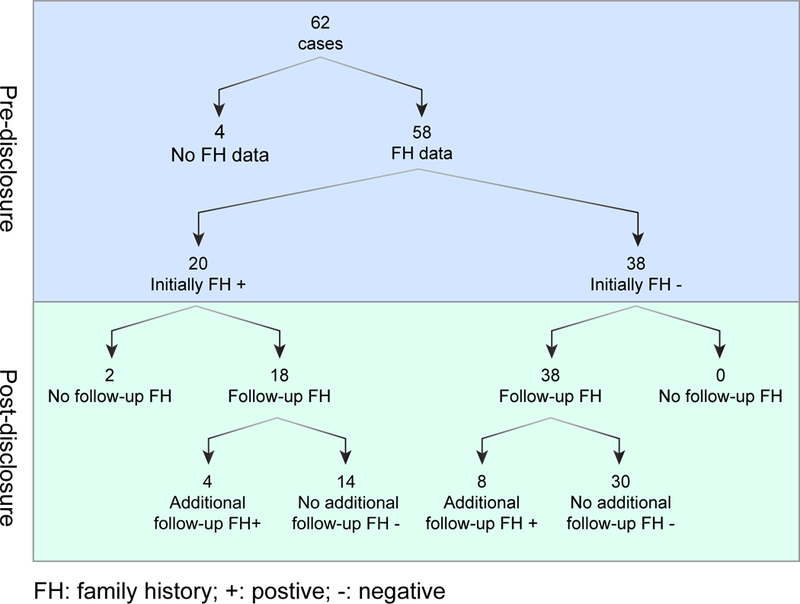
Results: The overall adjusted prevalence of SFs in the ACMG 56 genes across the CSER consortium was 1.7%. Initially 32% of the family histories were positive, and post disclosure, this increased to 48%. The average cost of follow-up medical actions per finding up to a 1-year period was $128 (observed, range: $0-$678) and $421 (recommended, range: $141-$1114). Case reports revealed variability in the frequency of and follow-up on medical recommendations patients received associated with each SF gene-condition pair. Participants did not report adverse psychosocial impact associated with receiving SFs; this was corroborated by 18 participant (or parent) interviews. All interviewed participants shared findings with relatives and reported that relatives did not pursue additional testing or care.
Conclusion: Our results suggest that disclosure of SFs shows little to no adverse impact on participants and adds only modestly to near-term health-care costs; additional studies are needed to confirm these findings.
Keywords: genomic sequencing; health-care resource utilization; secondary findings.
Conflict of interest statement
Conflict of Interest: LMA, BBB, CLB, JSB, KBB, KLB, KMB, SB, KDC, GMC, LKC, MCD, JNE, KME, CRF, AAG, MJG, KABG, LAH, MRH, GPJ, JJJ, JBK, TLK, WVK, KLL, ALM, CM, JO, EJR, AMS, NBS, ET, MLT, JLV, BSW, none; CSR and HLR are employed by a testing laboratory that offers commercially available sequencing. RCG receives compensation for consultation from AIA, Americord, Helix and Veritas; and is co-founder, advisor and equity holder in Genome Medical, Inc; and is employed by a testing laboratory that offers commercially available sequencing. LGB is an uncompensated advisor to the Illumina Corp, receives royalties from Genentech, Inc, and honoraria from Wiley-Blackwell. SEP is a member of the Scientific Advisory Panel of the Baylor Genetics Laboratory. DLV is a consultant to Roche Sequencing Systems.
Figures
References
-
- Biesecker LG, Green RC. Diagnostic clinical genome and exome sequencing. N Engl J Med. 2014;370(25):2418–2425. - PubMed
-
- Kalia SS, Adelman K, Bale SJ, et al. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 updated (ACMG SF v2.0): a policy statement of the American College of Medical Genetics and Genomics. Genetics in Medicine. 2017;19(2):249–255. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HG006546/HG/NHGRI NIH HHS/United States
- RF1 AG047866/AG/NIA NIH HHS/United States
- T15 LM007442/LM/NLM NIH HHS/United States
- U01 HG006507/HG/NHGRI NIH HHS/United States
- U01 HG006485/HG/NHGRI NIH HHS/United States
- U24 HG007307/HG/NHGRI NIH HHS/United States
- U01 HG010233/HG/NHGRI NIH HHS/United States
- U01 HG006500/HG/NHGRI NIH HHS/United States
- U01 HG007307/HG/NHGRI NIH HHS/United States
- IK2 CX001262/CX/CSRD VA/United States
- U01 HG007301/HG/NHGRI NIH HHS/United States
- K01 HG009173/HG/NHGRI NIH HHS/United States
- ZIA HG200359/ImNIH/Intramural NIH HHS/United States
- UM1 HG007292/HG/NHGRI NIH HHS/United States
- R01 CA154517/CA/NCI NIH HHS/United States
- ZIA HG200387/ImNIH/Intramural NIH HHS/United States
- UM1 HG007301/HG/NHGRI NIH HHS/United States
- U01 HG006487/HG/NHGRI NIH HHS/United States
- U01 HG006492/HG/NHGRI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
