

Antiretroviral therapy and liver disease progression in HIV and hepatitis C co-infected patients: a systematic review and meta-analysis
- PMID: 30288314
- PMCID: PMC5918754
- DOI: 10.1186/s41124-016-0015-7
Antiretroviral therapy and liver disease progression in HIV and hepatitis C co-infected patients: a systematic review and meta-analysis
Abstract
Background: HIV co-infection exacerbates hepatitis C disease, increasing the risk of cirrhosis and hepatitis C-related mortality. Combination antiretroviral therapy (cART) is the current standard treatment for co-infected individuals, but the impact of cART and antiretroviral (ARV) monotherapy on liver disease in this population is unclear. We aimed to assess the effect of cART and ARV monotherapy on liver disease progression and liver-related mortality in individuals co-infected with HIV and chronic hepatitis C.
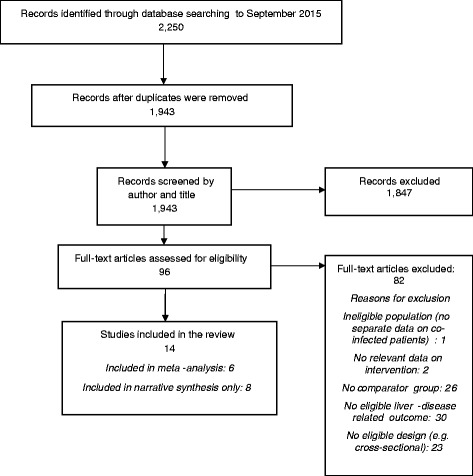
Methods: A systematic review with meta-analyses was conducted. MEDLINE and EMBASE bibliographic databases were searched up to September 2015. Study quality was assessed using a modified Newcastle-Ottawa scale. Results were synthesised narratively and by meta-analysis.
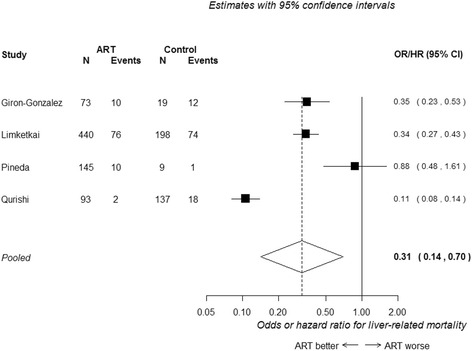
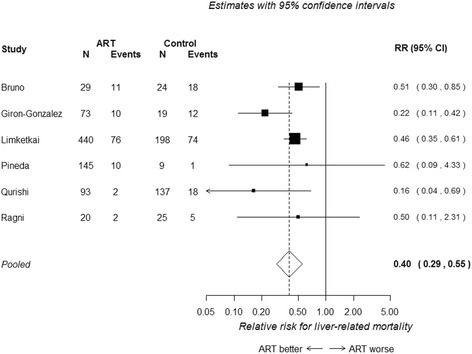
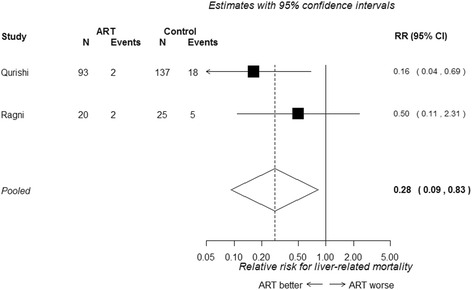
Results: Fourteen observational studies were included. In analyses that adjusted for potential confounders, risk of liver-related mortality was significantly lower in patients receiving cART (hazard ratio/odds ratio 0.31, 95 % CI 0.14 to 0.70). Results were similar in unadjusted analyses (relative risk 0.40, 95 % CI 0.29 to 0.55). For outcomes where meta-analysis could not be performed, results were less consistent. Some studies found cART was associated with lower incidence of, or slower progression of liver disease, fibrosis and cirrhosis, while others showed no evidence of benefit. We found no evidence of liver-related harm from cART or ARV monotherapy compared with no HIV therapy.
Conclusions: cART was associated with significantly lower liver-related mortality in patients co-infected with HIV and HCV. Evidence of a positive association between cART and/or ARV monotherapy and liver-disease progression was less clear, but there was no evidence to suggest that the absence of antiretroviral therapy was preferable.
Keywords: Anti-retroviral agents; HIV; Hepatitis C; Meta-analysis; Systematic review.
Conflict of interest statement
Will Irving has served as a speaker, a consultant and an advisory board member for Janssen Cilag, Bristol-Myers Squibb, and has received research funding from Gilead Sciences, Janssen Cilag and educational grants from Boehringer Ingelheim, Gilead Sciences and MSD. The authors declare they have no other competing interests.
Figures
References
-
- Platt L, Easterbrook P, Gower E, McDonald B, Sabin K, McGowan C et al. Prevalence and burden of HCV co-infection in people living with HIV: a global systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):797–808 - PubMed
-
- de Ledinghen V, Barreiro P, Foucher J, Labarga P, Castera L, Vispo ME, et al. Liver fibrosis on account of chronic hepatitis C is more severe in HIV-positive than HIV-negative patients despite antiretroviral therapy. J Viral Hepat. 2008;15(6):427–33. - PubMed
LinkOut - more resources
Full Text Sources