

Long-term outcomes of a phase I study of agonist CD40 antibody and CTLA-4 blockade in patients with metastatic melanoma
- PMID: 30288340
- PMCID: PMC6169575
- DOI: 10.1080/2162402X.2018.1468956
Long-term outcomes of a phase I study of agonist CD40 antibody and CTLA-4 blockade in patients with metastatic melanoma
Abstract
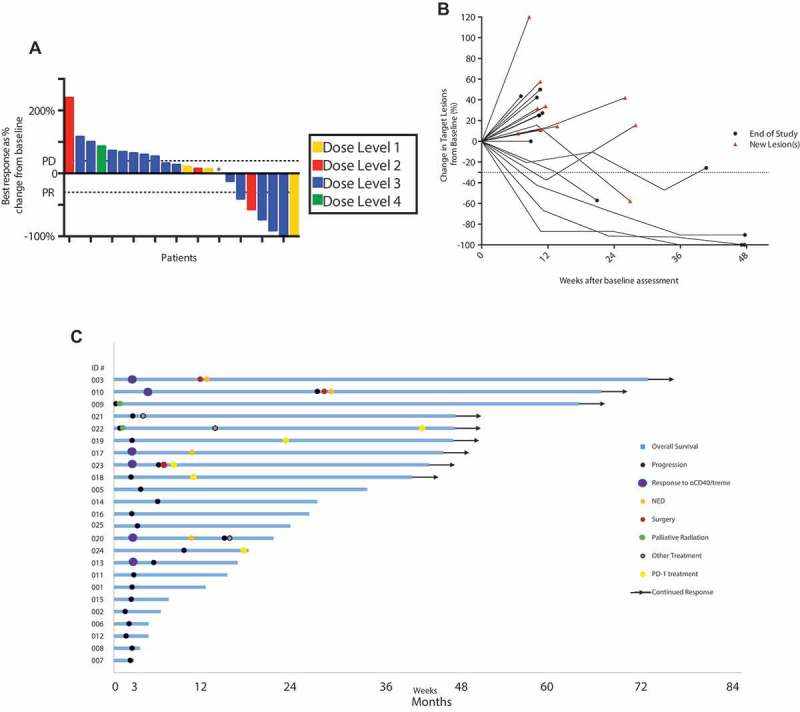
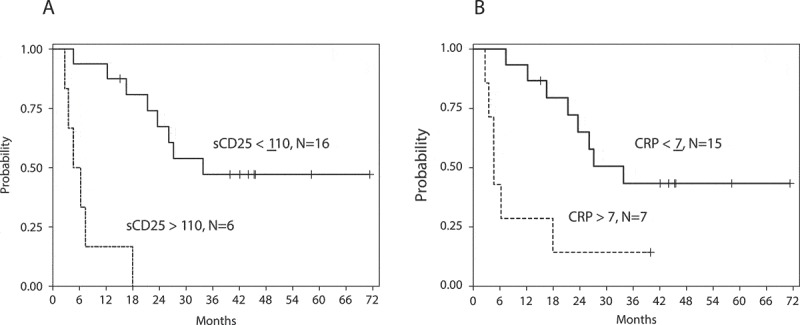
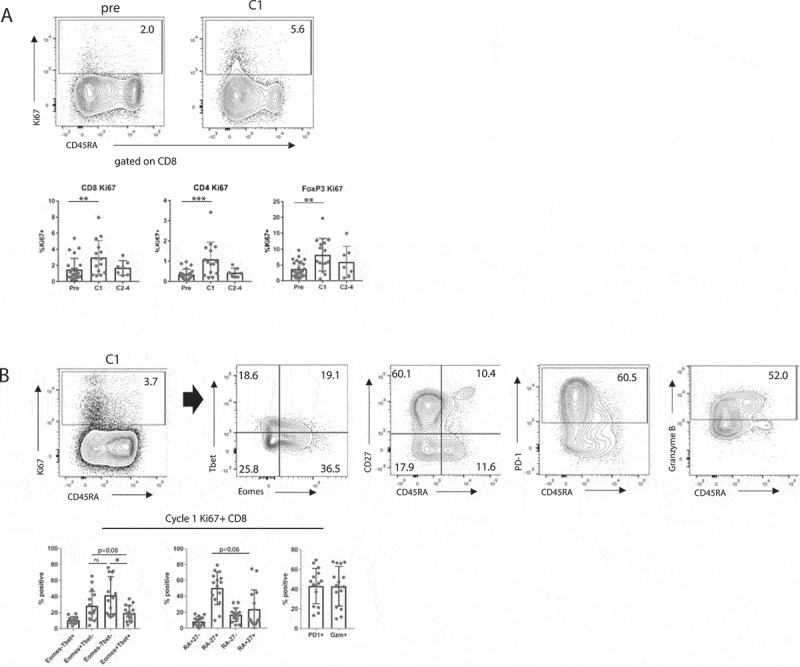
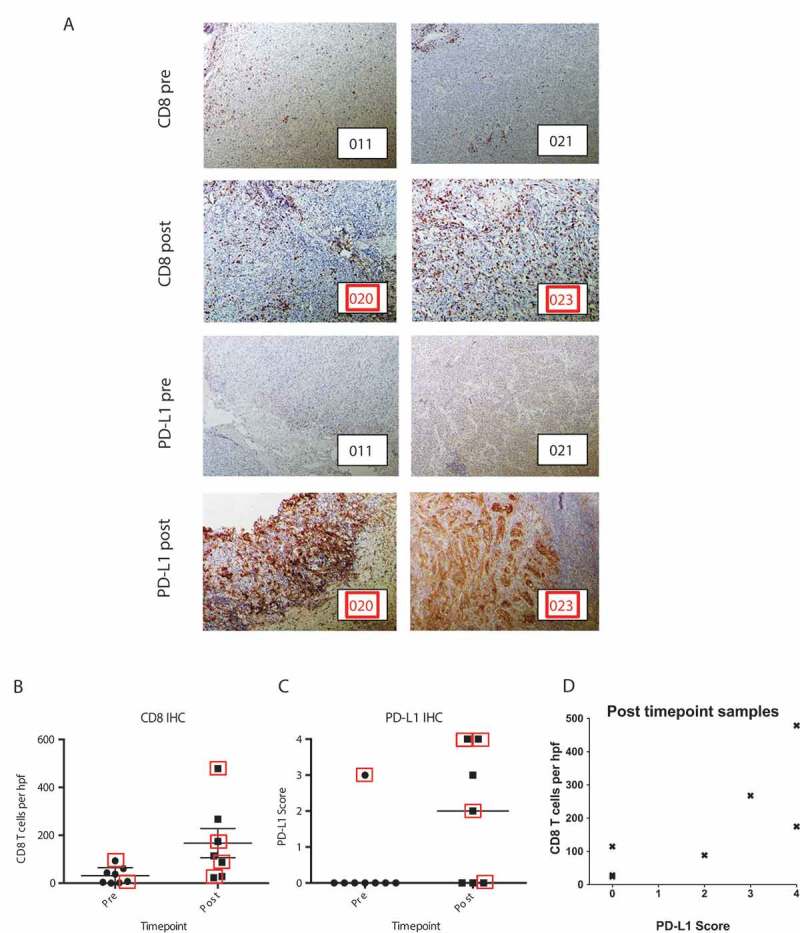
We report long-term clinical outcomes and immune responses observed from a phase 1 trial of agonist CD40 monoclonal antibody (mAb) and blocking CTLA-4 mAb in patients with metastatic melanoma. Twenty-four patients previously untreated with checkpoint blockade were enrolled. The agonistic CD40 mAb CP-870,893 and the CTLA-4 blocking mAb tremelimumab were dosed concomitantly every 3 weeks and 12 weeks, respectively, across four dose combinations. Two patients developed dose-limiting grade 3 immune-mediated colitis that led to the definition of the maximum tolerated dose (MTD). Other immune-mediated toxicity included uveitis (n = 1), hypophysitis (n = 1), hypothyroidism (n = 2), and grade 3 cytokine release syndrome (CRS) (n = 1). The estimated MTD was 0.2 mg/kg of CP-870,893 and 10 mg/kg of tremelimumab. In 22 evaluable patients, the objective response rate (ORR) was 27.3%: two patients (9.1%) had complete responses (CR) and four (18.2%) patients had partial responses (PR). With a median follow-up of 45 months, the median progression-free survival (PFS) was 3.2 months (95% CI, 1.3-5.1 months) and median overall survival (OS) was 23.6 months (95% CI, 11.7-35.5 months). Nine patients are long-term survivors (> 3 years), 8 of whom subsequently received other therapy including PD-1 mAb, surgery, or radiation therapy. Elevated baseline soluble CD25 was associated with shorter OS. Immunologically, treatment was associated with evidence of T cell activation and increased tumor T cell infiltration that was accomplished without therapeutic PD-1/PD-L1 blockade. These results suggest opportunities for immune activation and cancer immunotherapy beyond PD-1.
Keywords: CD40; CTLA4; melanoma.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous