

Uterine Artery Embolization in Women with Symptomatic Cervical Leiomyomata: Efficacy and Safety
- PMID: 30288591
- PMCID: PMC6373190
- DOI: 10.1007/s00270-018-2081-2
Uterine Artery Embolization in Women with Symptomatic Cervical Leiomyomata: Efficacy and Safety
Abstract
Purpose: To perform an evaluation on safety and efficacy of uterine artery embolization (UAE) in the patients with symptomatic cervical leiomyomata.
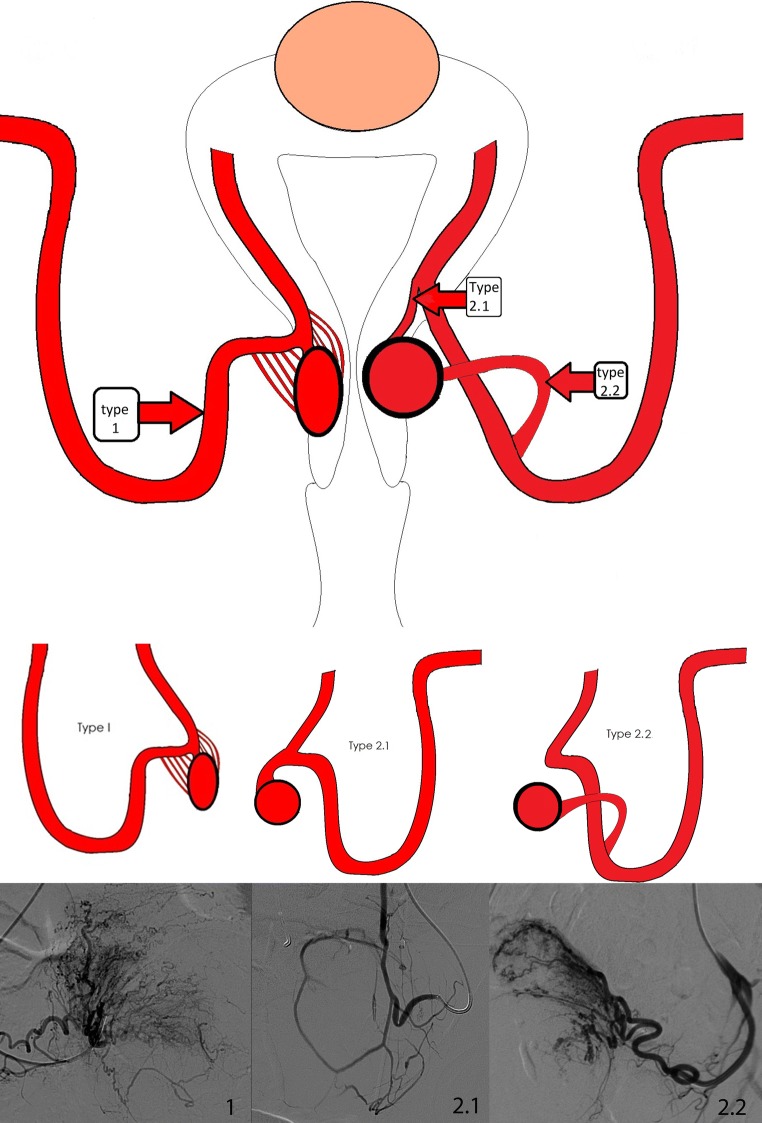
Methods: Patients with symptomatic cervical leiomyomata who underwent UAE in one specialized hospital were retrospectively analyzed, both clinically and with MR imaging. The 3-month outcomes were assessed with MR imaging and a validated questionnaire. Long-term follow-up was assessed by direct contact or file review. To determine the efficacy of UAE for cervical leiomyomata, the primary objective was to assess the clinical outcome with the UFS-QOL questionnaire, containing the health-related quality of life (HRQOL) and symptom severity score (SSS). To assess safety, the secondary objective included leiomyomata volume reduction, the infarction/complication rate and secondary interventions were needed.
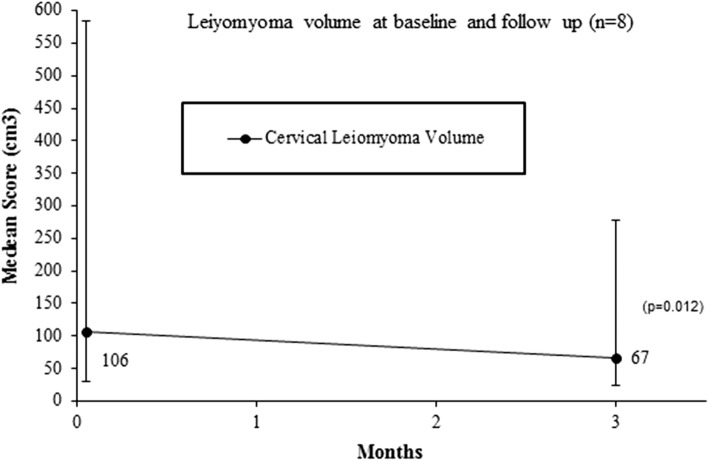
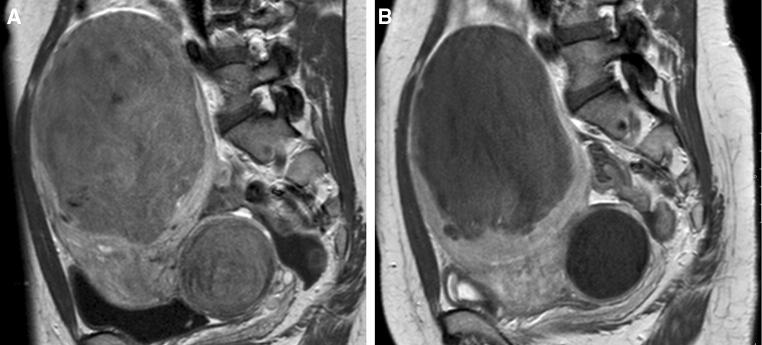
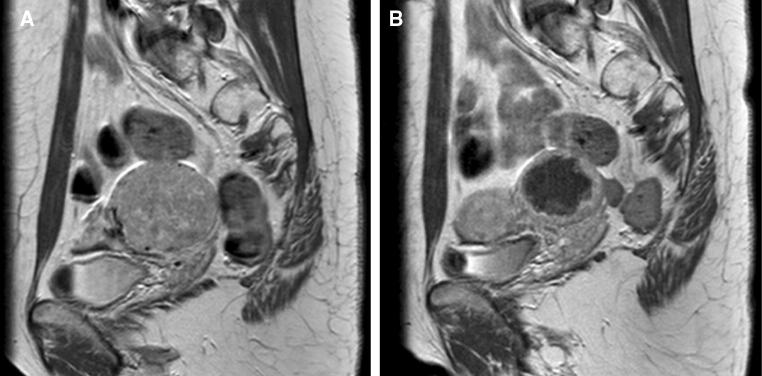
Results: Between 2006 and 2017, eight of 1180 patients underwent UAE and were eligible for inclusion. All embolizations were technically successful (n = 8). At 3 months, all patients showed cervical leiomyomata volume reduction with a median reduction of 41.5% (38.8 cm3) compared to baseline (p = 0.012). No complications occurred. At a median follow-up of 3 months (range 1-7, n = 7), the HRQOL and SSS improved with a median difference of 13 points (range - 5 to 60, p = 0.063) and - 13 points (range - 79 to 3, p = 0.046), respectively. Long-term follow-up showed two secondary interventions (median of 43.5 months). Six patients reported no symptom recurrence.
Conclusion: UAE in women with symptomatic cervical leiomyomata is effective and safe with significant improvement in symptoms and quality of life. UAE is a valuable option for women seeking a non-surgical solution.
Keywords: Cervical leiomyomata; Health-related quality of life (HRQOL); Uterine artery embolization.
Conflict of interest statement
Dr. P.N.M. Lohle has a consultancy agreement with Boston Scientific. All other authors declare that they have no conflicts of interest.
Figures

References
-
- Stovall T. Myomectomy. In: Mann WJ, Stovall T, editors. Gynecologic surgery. New York: Churchill Livingstone; 1996. pp. 445–461.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
