

Extended follow-up for prostate cancer incidence and mortality among participants in the Prostate, Lung, Colorectal and Ovarian randomized cancer screening trial
- PMID: 30288918
- PMCID: PMC6450783
- DOI: 10.1111/bju.14580
Extended follow-up for prostate cancer incidence and mortality among participants in the Prostate, Lung, Colorectal and Ovarian randomized cancer screening trial
Abstract
Objective: To examine prostate cancer (PCa) incidence and mortality by arm in the randomized Prostate, Lung, Colorectal and Ovarian (PLCO) cancer screening trial.
Patients and methods: Patients aged 55-74 years at 10 screening centres were randomized between 1993 and 2001 to an intervention or usual care arm. Patients in the intervention arm received six annual prostate-specific antigen (PSA) tests and four annual digital rectal examinations. The patients were followed for PCa incidence and for mortality via active follow-up processes and by linkage to state cancer registries and the National Death Index. For cancers identified through active follow-up, trial abstractors recorded the mode of diagnosis (screen-detected, symptomatic, other).
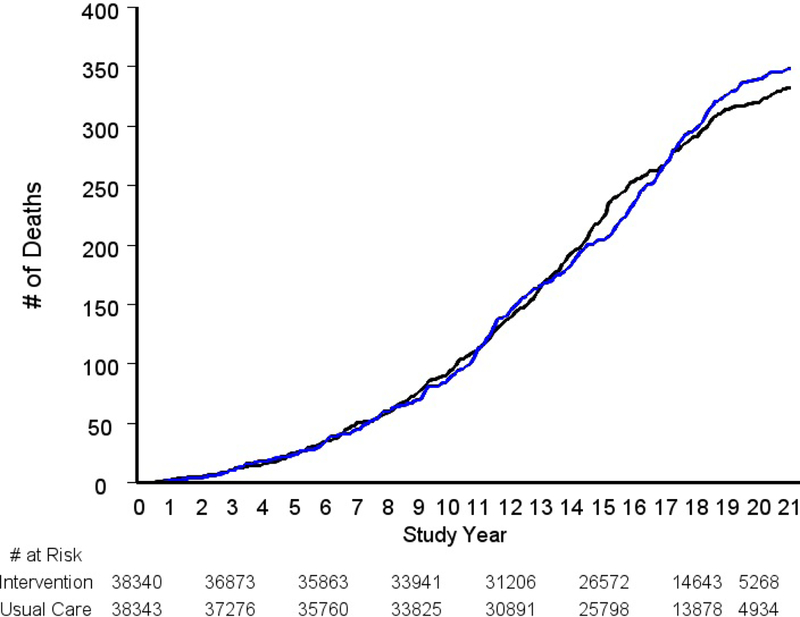
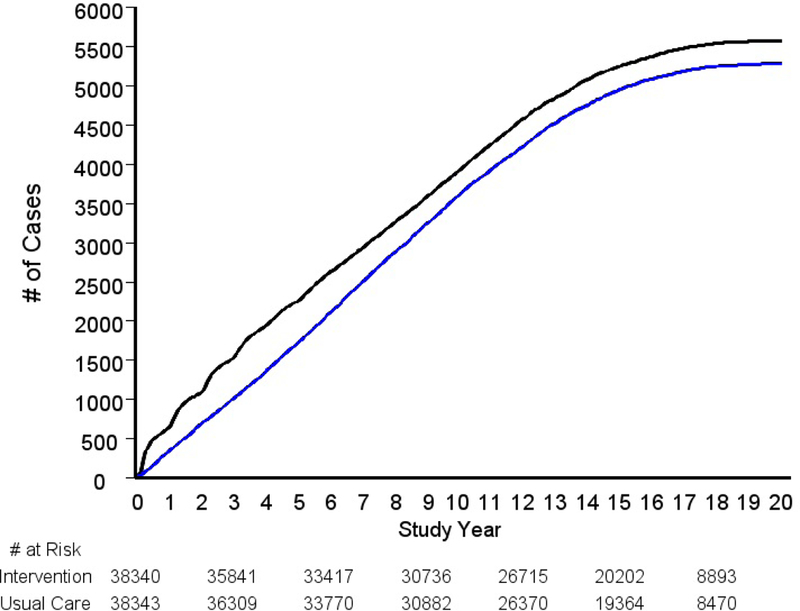
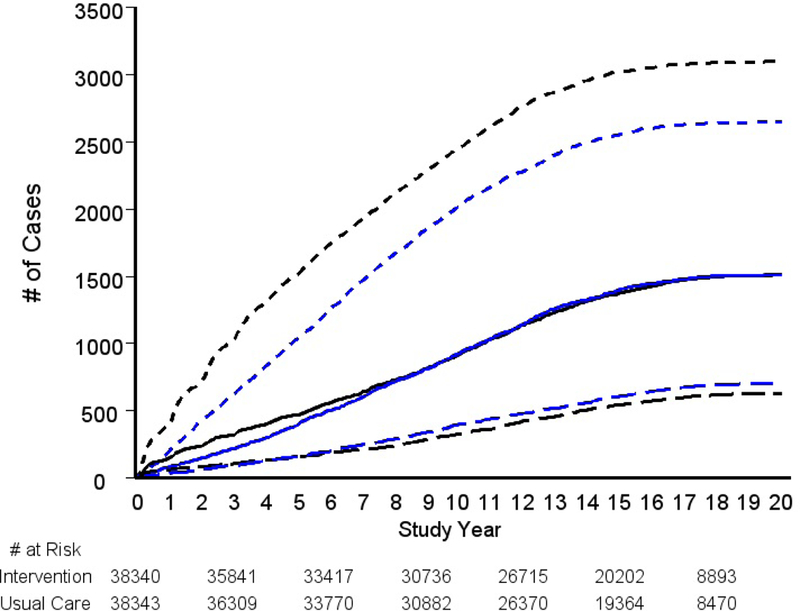
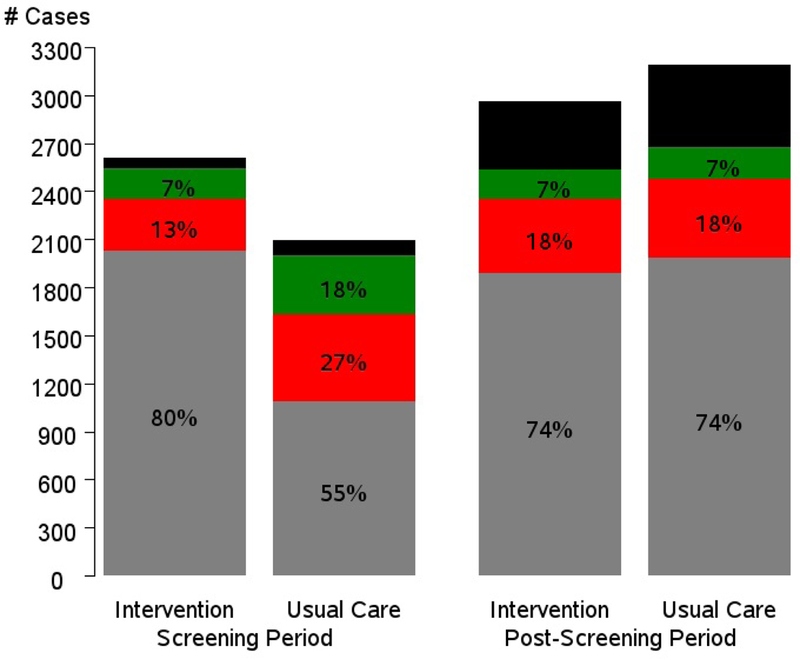
Results: A total of 38 340 patients were randomized to the intervention arm and 38 343 to a usual care arm. The median follow-up for mortality was 16.9 (intervention) and 16.7 years (usual care). There were 333 (intervention) and 352 (usual care) PCa cancer deaths, giving rates (per 10 000 person-years) of 5.5 and 5.9, respectively, and a rate ratio (RR) of 0.93 (95% confidence interval [CI] 0.81-1.08; P = 0.38). The RR for overall PCa incidence was 1.05 (95% CI 1.01-1.09). The RRs by Gleason category were 1.17 (95% CI 1.11-1.23) for Gleason 2-6, 1.00 (95% CI 0.93-1.07) for Gleason 7 and 0.89 (95% CI 0.80-0.99) for Gleason 8-10 disease. By mode of detection, during the trial's screening phase, 13% of intervention arm vs 27% of usual care arm cases were symptomatic; post-screening, these percentages were 18% in each arm.
Conclusion: After almost 17 years of median follow-up, there was no significant reduction in PCa mortality in the intervention compared with the usual care arm. There was a significant increase in Gleason 2-6 disease and a significant reduction in Gleason 8-10 disease in the intervention compared with the usual care arm.
Keywords: #PCSM; #ProstateCancer; #uroonc; prostate-specific antigen; screening.
© 2018 The Authors BJU International © 2018 BJU International Published by John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Schroder FH, Hugosson J, Roobol MJ, et al. Screening and prostate cancer mortality in a randomized European study. New Engl J Med 2010; 360: 1320–1328. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
