

Magnetic Resonance Elastography of Liver: Current Update
- PMID: 30289828
- PMCID: PMC6176736
- DOI: 10.1097/RMR.0000000000000177
Magnetic Resonance Elastography of Liver: Current Update
Abstract
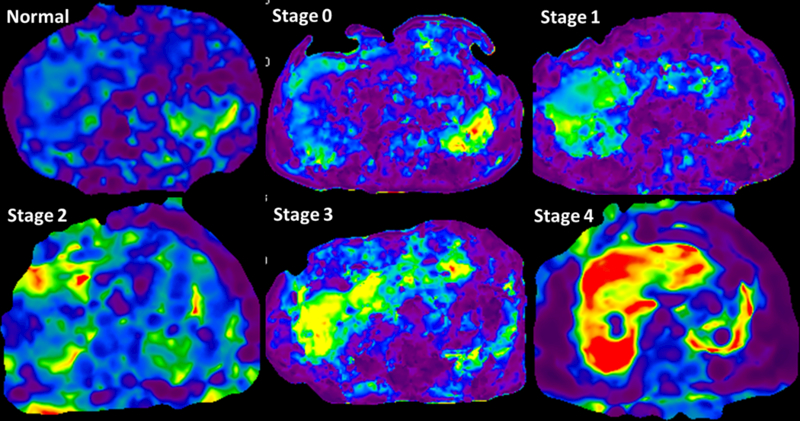
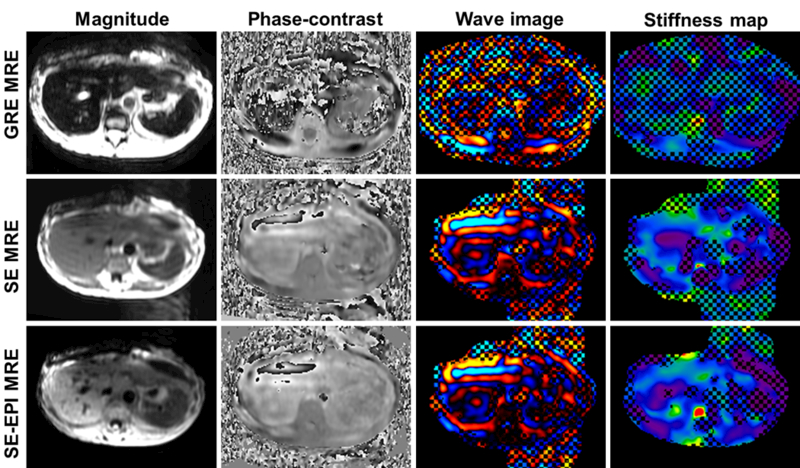
The first clinical application of magnetic resonance elastography (MRE) was in the evaluation of chronic liver disease (CLD) for detection and staging of liver fibrosis. In the past 10 years, MRE has been incorporated seamlessly into a standard magnetic resonance imaging (MRI) liver protocol worldwide. Liver MRE is a robust technique for evaluation of liver stiffness and is currently the most accurate noninvasive imaging technology for evaluation of liver fibrosis. Newer MRE sequences including spin-echo MRE and 3 dimensional MRE have helped in reducing the technical limitations of clinical liver MRE that is performed with 2D gradient recalled echo (GRE) MRE. Advances in MRE technology have led to understanding of newer mechanical parameters such as dispersion, attenuation, and viscoelasticity that may be useful in evaluating pathological processes in CLD and may prove useful in their management.This review article will describe the changes in CLD that cause an increase in stiffness followed by principle and technique of liver MRE. In the later part of the review, we will briefly discuss the advances in liver MRE.
Figures
References
-
- Kim WR, Brown RS Jr., Terrault NA, El-Serag H. Burden of liver disease in the United States: summary of a workshop. Hepatology (Baltimore, Md) 2002;36(1):227–42. - PubMed
-
- Tsuchida T, Friedman SL. Mechanisms of hepatic stellate cell activation. Nature reviews Gastroenterology & hepatology 2017;14(7):397–411. - PubMed
-
- EASL clinical practice guidelines: Management of chronic hepatitis B virus infection. J Hepatol 2012;57(1):167–85. - PubMed
-
- Cadranel JF, Rufat P, Degos F. Practices of liver biopsy in France: results of a prospective nationwide survey. For the Group of Epidemiology of the French Association for the Study of the Liver (AFEF). Hepatology (Baltimore, Md) 2000;32(3):477–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
