

A Paradigm Shift in Cancer Immunotherapy: From Enhancement to Normalization
- PMID: 30290139
- PMCID: PMC6538253
- DOI: 10.1016/j.cell.2018.09.035
A Paradigm Shift in Cancer Immunotherapy: From Enhancement to Normalization
Erratum in
-
A Paradigm Shift in Cancer Immunotherapy: From Enhancement to Normalization.Cell. 2019 Jan 24;176(3):677. doi: 10.1016/j.cell.2019.01.008. Cell. 2019. PMID: 30682374 No abstract available.
Abstract
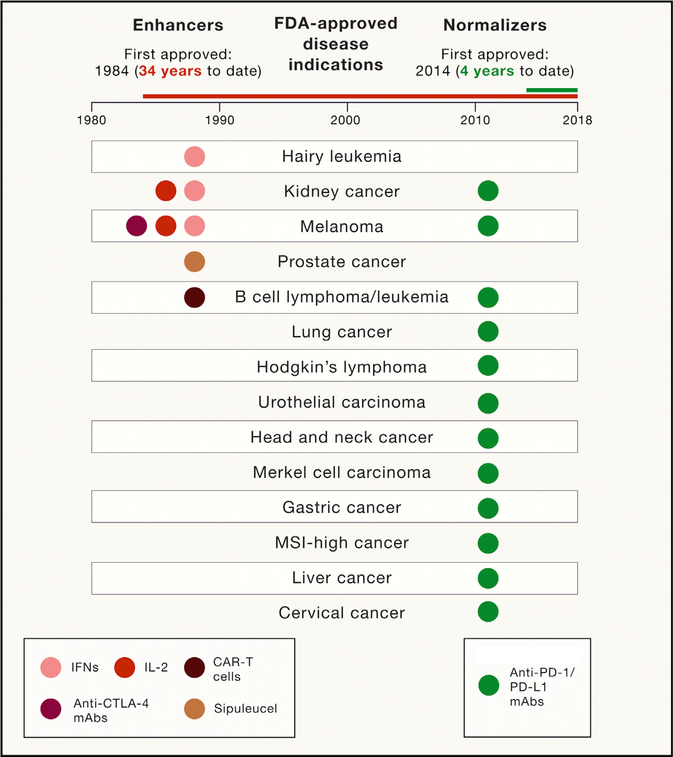
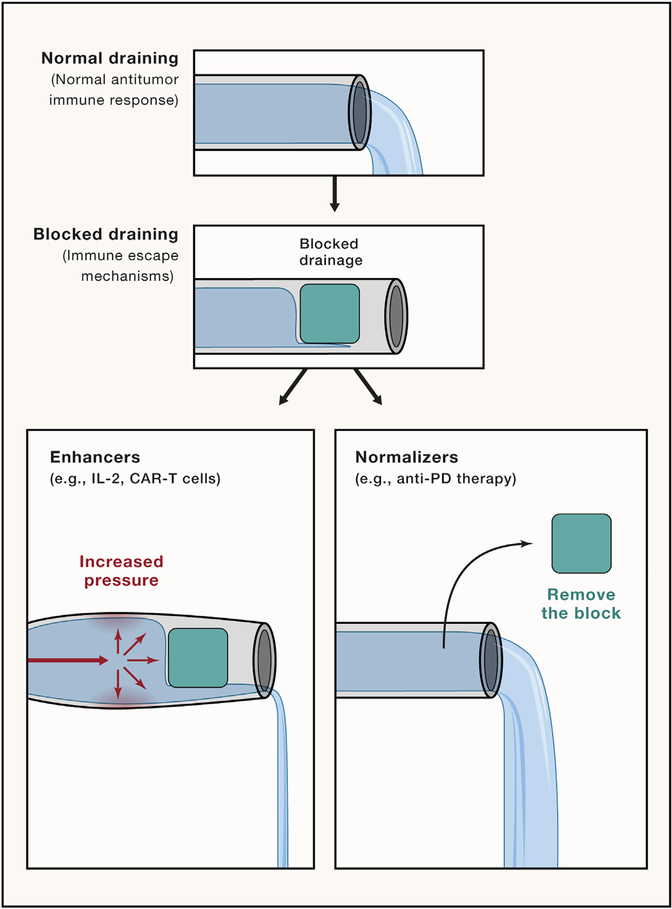
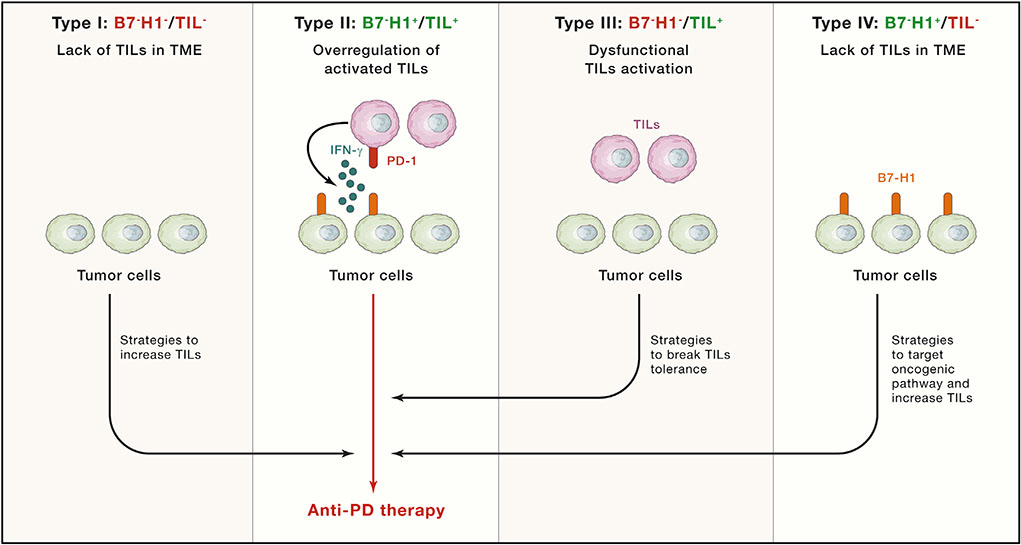
Harnessing an antitumor immune response has been a fundamental strategy in cancer immunotherapy. For over a century, efforts have primarily focused on amplifying immune activation mechanisms that are employed by humans to eliminate invaders such as viruses and bacteria. This "immune enhancement" strategy often results in rare objective responses and frequent immune-related adverse events (irAEs). However, in the last decade, cancer immunotherapies targeting the B7-H1/PD-1 pathway (anti-PD therapy), have achieved higher objective response rates in patients with much fewer irAEs. This more beneficial tumor response-to-toxicity profile stems from distinct mechanisms of action that restore tumor-induced immune deficiency selectively in the tumor microenvironment, here termed "immune normalization," which has led to its FDA approval in more than 10 cancer indications and facilitated its combination with different therapies. In this article, we wish to highlight the principles of immune normalization and learn from it, with the ultimate goal to guide better designs for future cancer immunotherapies.
Keywords: B7-H1; PD-1; PD-L1; cancer; immunotherapy; normalization.
Copyright © 2018. Published by Elsevier Inc.
Figures
References
-
- Agarwala SS, Glaspy J, O’Day SJ, Mitchell M, Gutheil J, Whitman E, Gonzalez R, Hersh E, Feun L, Belt R, et al. (2002). Results from a randomized phase III study comparing combined treatment with histamine dihydrochloride plus interleukin-2 versus interleukin-2 alone in patients with metastatic melanoma. J. Clin. Oncol 20, 125–133. - PubMed
-
- Ahmed N, Brawley VS, Hegde M, Robertson C, Ghazi A, Gerken C, Liu E, Dakhova O, Ashoori A, Corder A, et al. (2015). Human Epidermal Growth Factor Receptor 2 (HER2) -Specific Chimeric Antigen Receptor-Modified T Cells for the Immunotherapy of HER2-Positive Sarcoma. J. Clin. Oncol 33, 1688–1696. - PMC - PubMed
-
- Ascierto PA, Del Vecchio M, Robert C, Mackiewicz A, Chiarion-Sileni V, Arance A, Lebbé C, Bastholt L, Hamit O, Rutkowski P, et al. (2017). Ipilimumab 10 mg/kg versus ipilimumab 3 mg/kg in patients with unresectable or metastaticmelanoma: a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 18, 611–622. - PubMed
-
- Atkins MB, Lotze MT, Dutcher JP, Fisher RI, Weiss G, Margolin K, Abrams J, Sznol M, Parkinson D, Hawkins M, et al. (1999). High-dose recombinant interleukin 2 therapy for patients with metastatic melanoma: analysis of 270 patients treated between 1985 and 1993. J. Clin. Oncol 17, 2105–2116. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
