

Selection of pancreaticojejunostomy technique after pancreaticoduodenectomy: duct-to-mucosa anastomosis is not better than invagination anastomosis: A meta-analysis
- PMID: 30290634
- PMCID: PMC6200508
- DOI: 10.1097/MD.0000000000012621
Selection of pancreaticojejunostomy technique after pancreaticoduodenectomy: duct-to-mucosa anastomosis is not better than invagination anastomosis: A meta-analysis
Abstract
Background: One of the most clinically significant current discussions is the optimal pancreaticojejunostomy (PJ) technique for pancreaticoduodenectomy (PD). We performed a meta-analysis to compare duct-to-mucosa and invagination techniques for pancreatic anastomosis after PD.
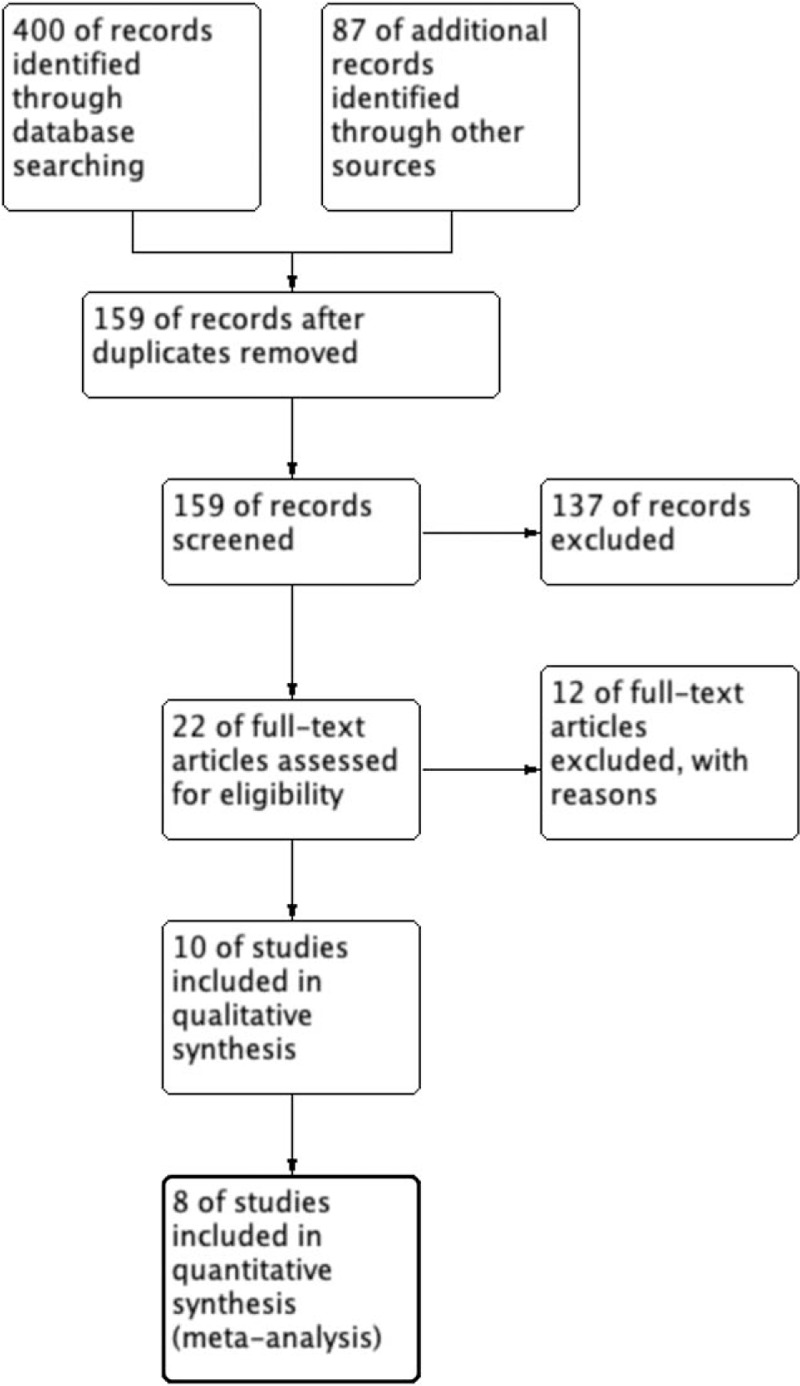
Methods: A systematic search of PubMed, Embase, Web of Science, the Cochrane Central Library, and ClinicalTrials.gov up to June 1, 2018 was performed. Randomized controlled trials (RCTs) comparing duct-to-mucosa versus invagination PJ were included. Statistical analysis was performed using RevMan 5.3 software.
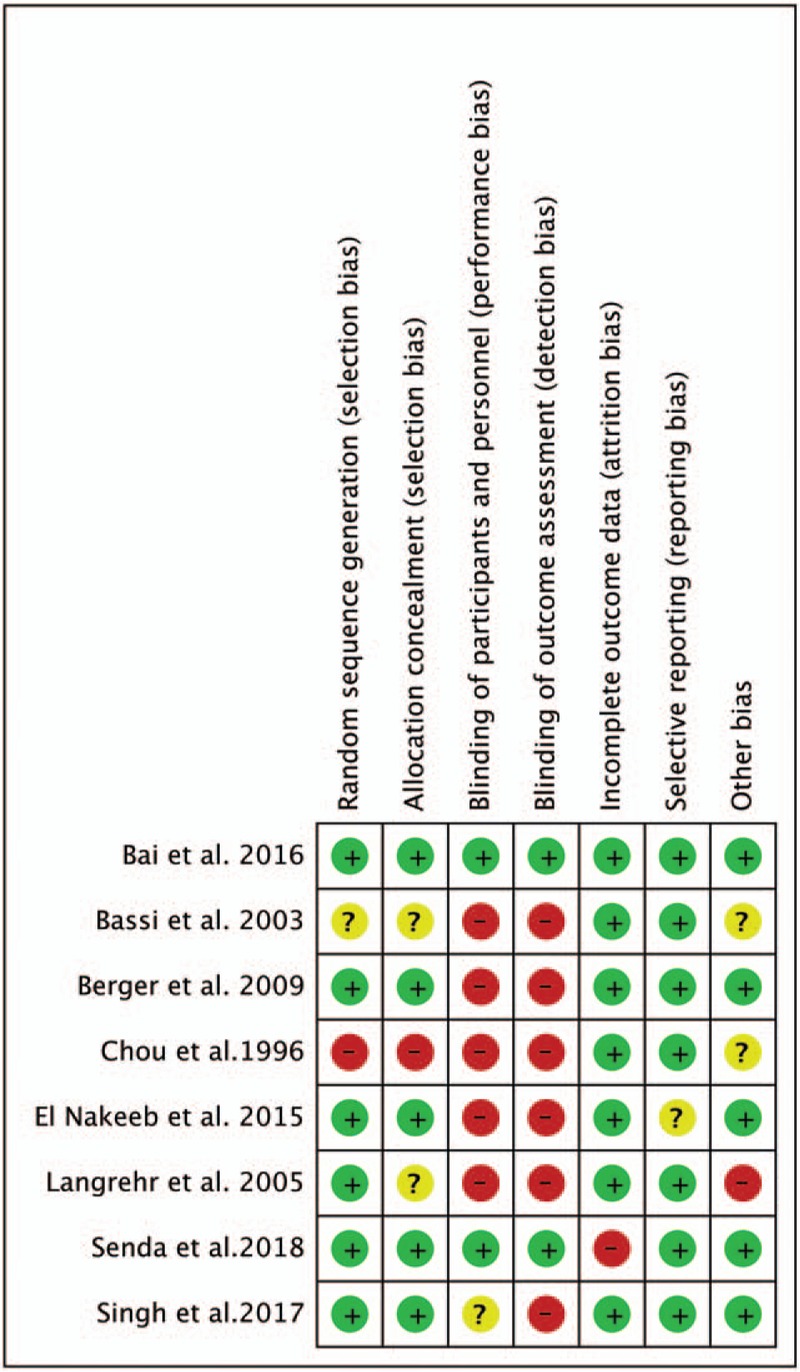
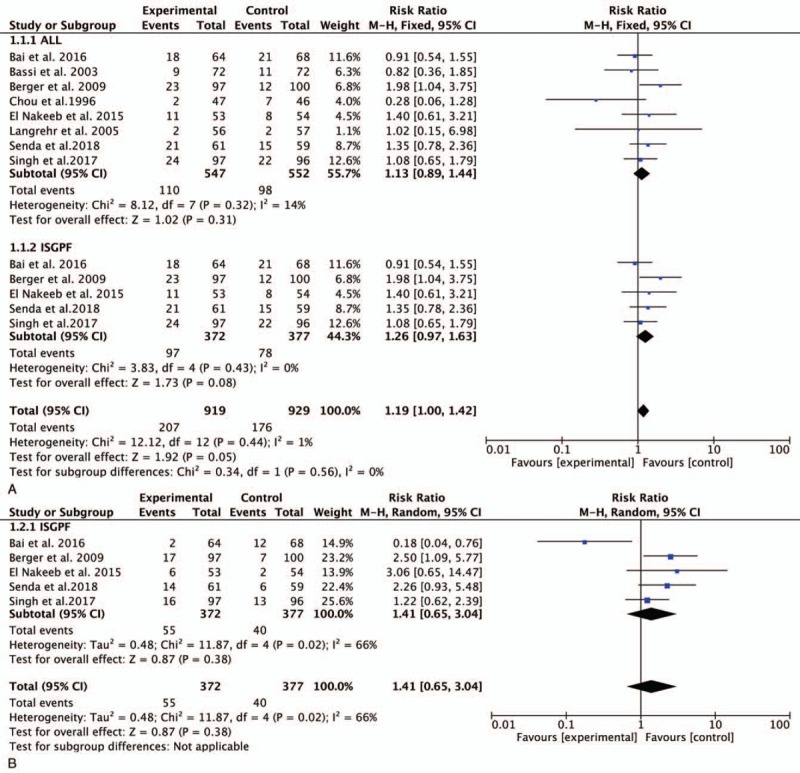
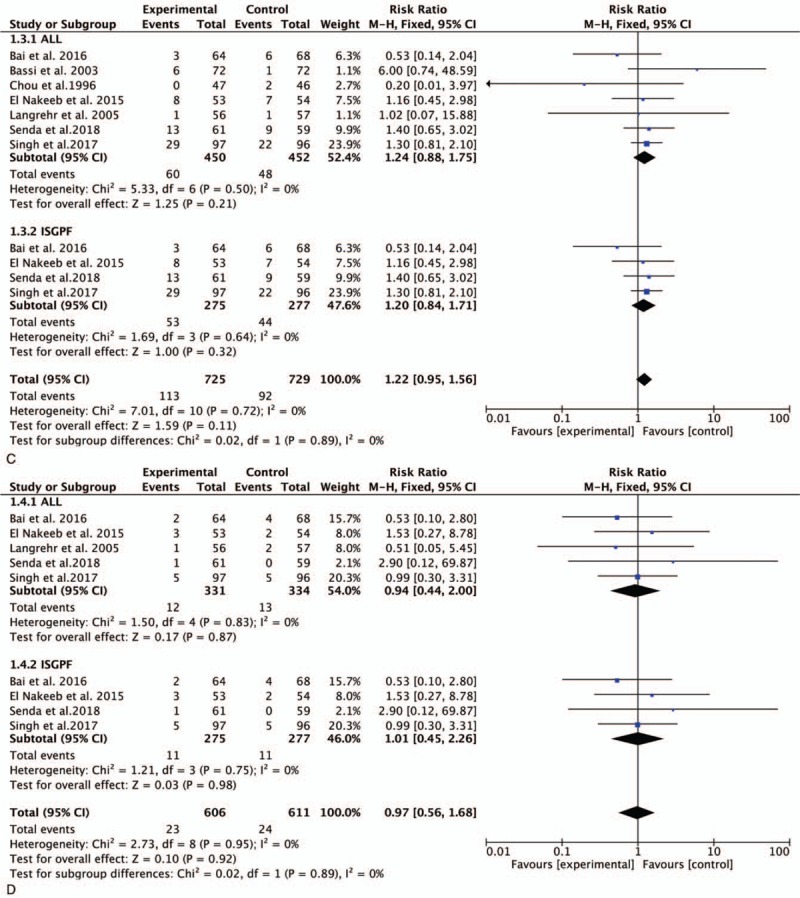
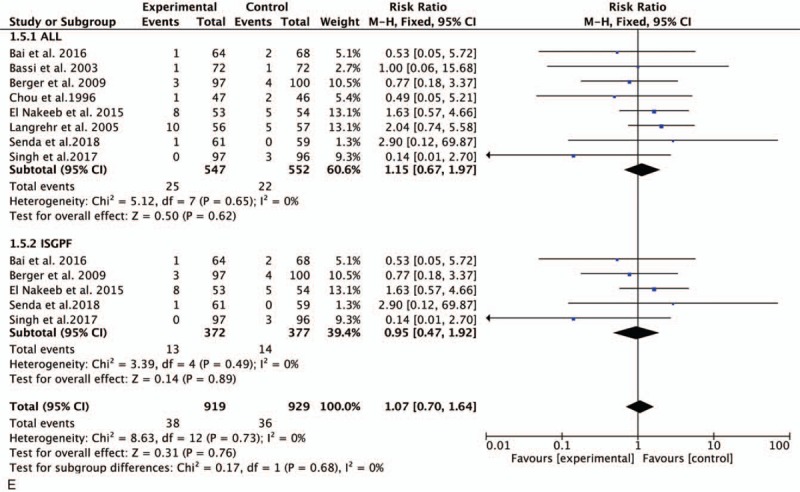
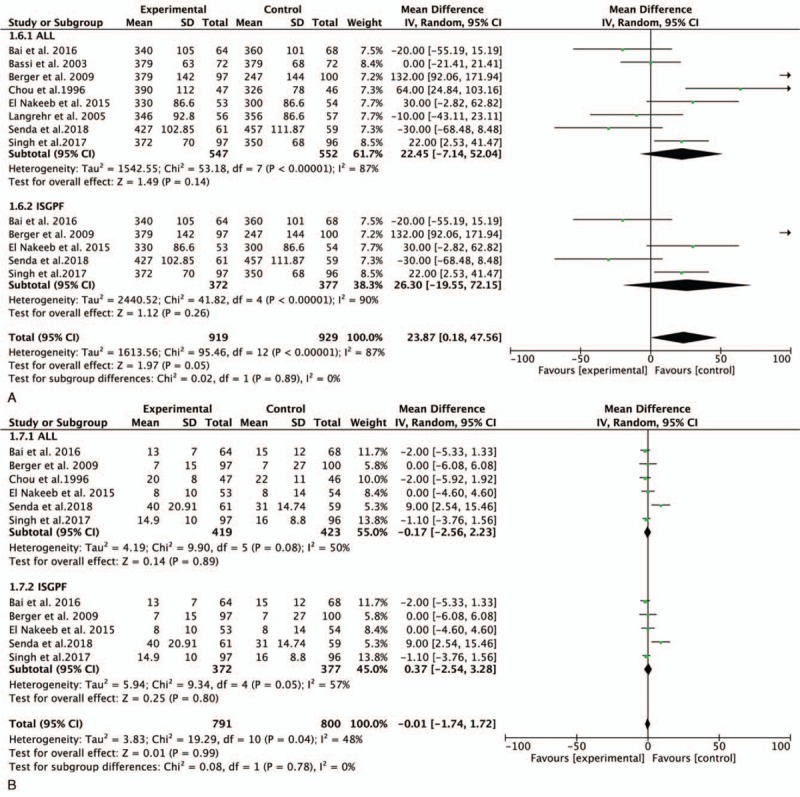
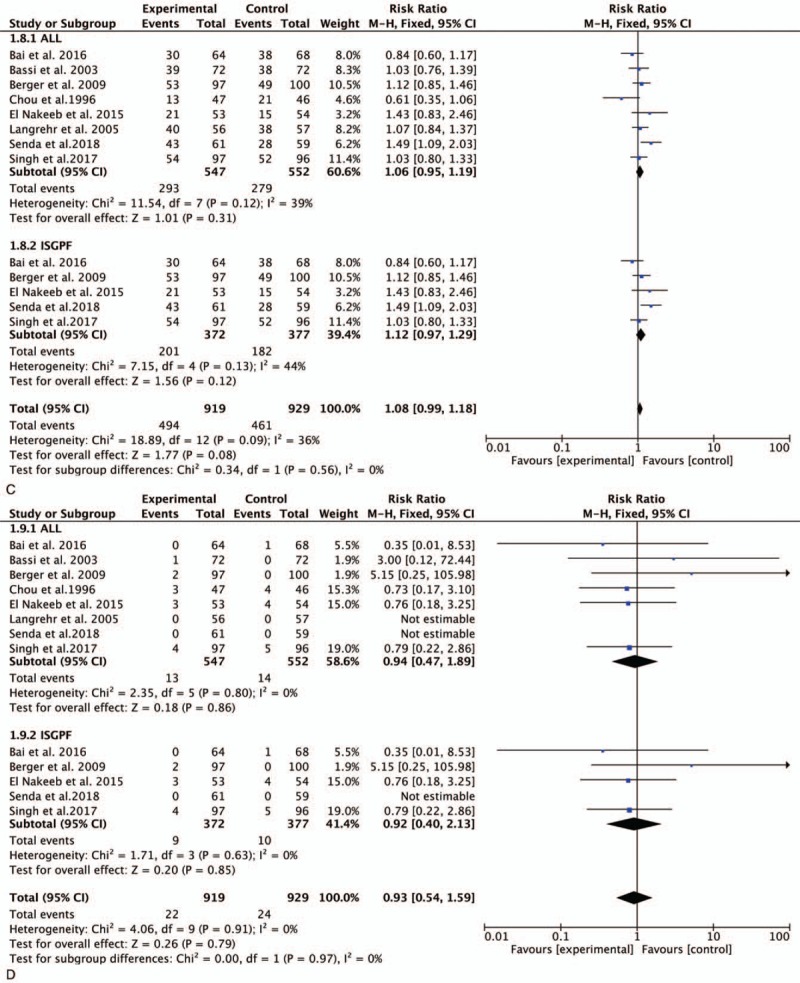
Results: Eight RCTs involving 1099 patients were included in the meta-analysis. The rate of postoperative pancreatic fistula (POPF) was not significantly different between the duct-to-mucosa PJ (110/547, 20.10%) and invagination PJ (98/552, 17.75%) groups in all 8 studies (risk ratio, 1.13; 95% CI, 0.89-1.44; P = .31). The subgroup analysis using the International Study Group on Pancreatic Fistula criteria showed no significant difference in POPF between duct-to-mucosa PJ (97/372, 26.08%) and invagination PJ (78/377, 20.68%). No significant difference in clinically relevant POPF (CR-POPF) was found between the 2 groups (55/372 vs 40/377, P = .38). Additionally, no significant differences in delayed gastric emptying, post-pancreatectomy hemorrhage, reoperation, operation time, or length of stay were found between the 2 groups. The overall morbidity and mortality rates were not significantly different between the 2 groups.
Conclusion: The duct-to-mucosa technique seems no better than the invagination technique for pancreatic anastomosis after PD in terms of POPF, CR-POPF, and other main complications. Further studies on this topic are therefore recommended.
Conflict of interest statement
All authors have declared that no competing interests exist. And all data and materials in this work were available from publications.
Figures
References
-
- Figueras J, Sabater L, Planellas P, et al. Randomized clinical trial of pancreaticogastrostomy versus pancreaticojejunostomy on the rate and severity of pancreatic fistula after pancreaticoduodenectomy. Br J Surg 2013;100:1597–605. - PubMed
-
- Topal B, Fieuws S, Aerts R, et al. Pancreaticojejunostomy versus pancreaticogastrostomy reconstruction after pancreaticoduodenectomy for pancreatic or periampullary tumours: a multicentre randomised trial. Lancet Oncol 2013;14:655–62. - PubMed
-
- Muscari F, Suc B, Kirzin S, et al. Risk factors for mortality and intra-abdominal complications after pancreatoduodenectomy: multivariate analysis in 300 patients. Surgery 2006;139:591–8. - PubMed
-
- Winter JM, Cameron JL, Campbell KA, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. J Gastrointest Surg 2006;10:1199–211. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
