

Role of qSOFA in predicting mortality of pneumonia: A systematic review and meta-analysis
- PMID: 30290639
- PMCID: PMC6200542
- DOI: 10.1097/MD.0000000000012634
Role of qSOFA in predicting mortality of pneumonia: A systematic review and meta-analysis
Abstract
Background: The concept of sepsis was redefined recently, and a new screening system termed the quick Sequential Organ Failure Assessment (qSOFA) was recommended for identifying infected patients at high risk for death. However, the predictive value of qSOFA for mortality in patients with pneumonia remains unclear. Thus, we performed a meta-analysis with the aim of determining the prognostic value of qSOFA in predicting mortality in patients with pneumonia.
Methods: Embase, Google Scholar, and PubMed (up to March 2018) were searched for related articles. We constructed a 2 × 2 contingency table according to mortality and qSOFA scores (<2 and ≥2) in patients with pneumonia. Two investigators independently extracted data and assessed study eligibility. A bivariate meta-analysis model was used to determine the prognostic value of qSOFA in predicting mortality. I index and Q-test were used to assess heterogeneity.
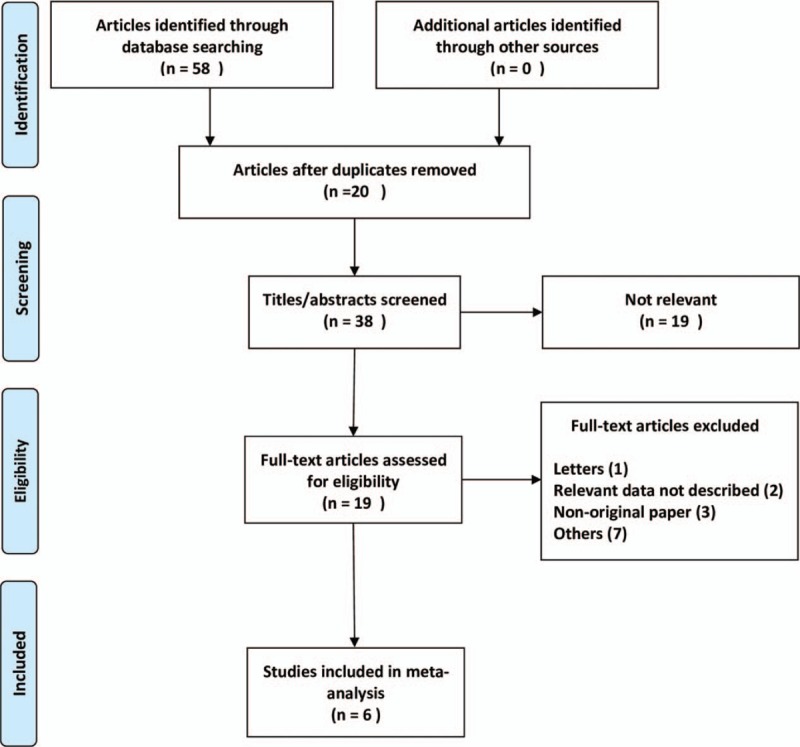
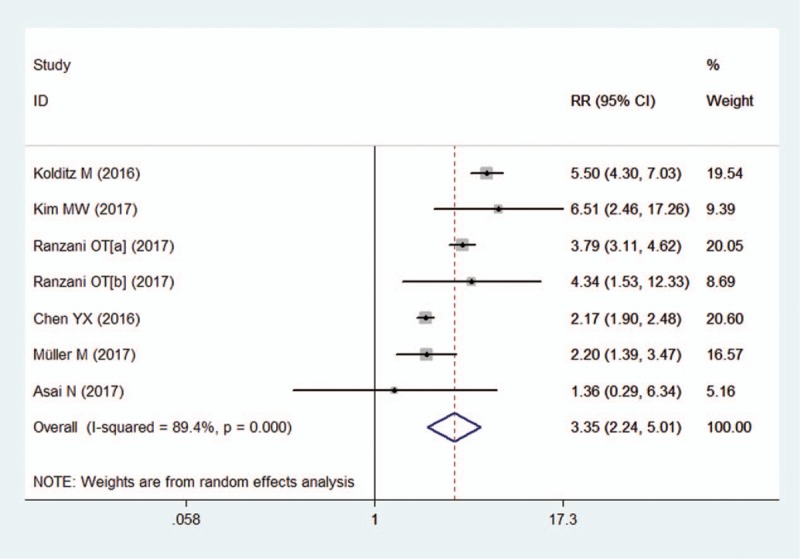
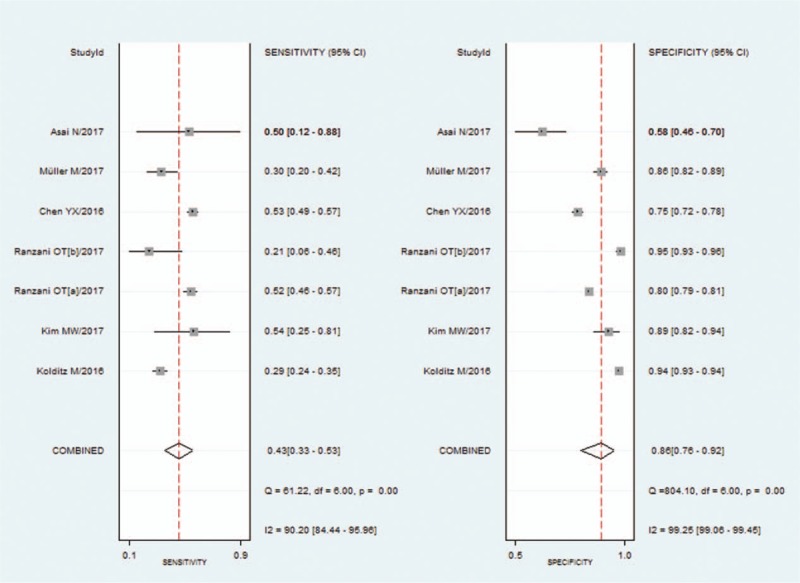
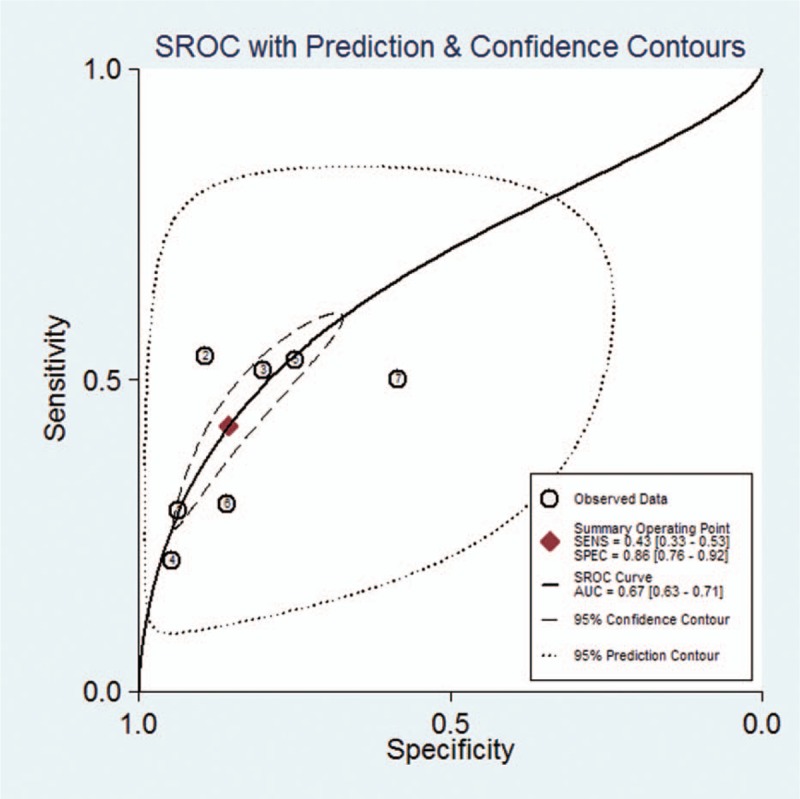
Results: Six studies with 17,868 patients were included. A qSOFA score ≥2 was related to a higher risk for death in patients with pneumonia, with a pooled risk ratio (RR) was 3.35 (95% CI, 2.24-5.01) using a random-effects model (I = 89.4%). The pooled sensitivity and specificity of a qSOFA score ≥2 to predict mortality in patients with pneumonia were 0.43 (95% CI, 0.33-0.53) and 0.86 (95% CI, 0.76-0.92), respectively. The diagnostic OR was 4 (95% CI, 3-6). The area under the summary receiver operator characteristic (SROC) curve was 0.67 (95% CI, 0.63-0.71). When we calculated the community-acquired pneumonia (CAP) subgroup, the pooled sensitivity and specificity were 0.36 (95% CI, 0.26-0.48) and 0.91 (95% CI, 0.84-0.95), respectively. The area under the SROC curve was 0.70 (95% CI, 0.66-0.74).
Conclusions: A qSOFA score ≥2 is strongly associated with mortality in patients with pneumonia, but the poor sensitivity of qSOFA may have limitations in the early identification of mortality in patients with pneumonia.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Guest JF, Morris A. Community-acquired pneumonia: the annual cost to the National Health Service in the UK. Eur Respir J 1997;10:1530–4. - PubMed
-
- Alberti C, Brun-Buisson C, Chevret S, et al. Systemic inflammatory response and progression to severe sepsis in critically ill infected patients. Am J Respir Crit Care Med 2005;171:461–8. - PubMed
-
- Restrepo MI, Jorgensen JH, Mortensen EM, et al. Severe community-acquired pneumonia: current outcomes, epidemiology, etiology, and therapy. Curr Opin Infect Dis 2001;14:703–9. - PubMed
-
- Dremsizov T, Clermont G, Kellum JA, et al. Severe sepsis in community-acquired pneumonia: when does it happen, and do systemic inflammatory response syndrome criteria help predict course? Chest 2006;129:968–78. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
