

Conventional immunosuppressive therapy in severe Behcet's Uveitis: the switch rate to the biological agents
- PMID: 30290779
- PMCID: PMC6173844
- DOI: 10.1186/s12886-018-0929-5
Conventional immunosuppressive therapy in severe Behcet's Uveitis: the switch rate to the biological agents
Abstract
Background: To report the switch rate of conventional immunosuppressive (CIS) therapies to the biological agents (BA) in patients with refractory Behcet's uveitis (BU).
Methods: In this retrospective study, clinical records were reviewed of 76 patients' 116 eyes presenting with BU who had been treated with immunosuppressive drug therapy. Mann Whitney U test was used for the intergroup comparisons of parameters without normal distribution as well as calculation of descriptive statistical methods (mean, standard deviation, median, frequency and rate). Wilcoxon Signed Ranks test was used for the intragroup comparisons of parameters without normal distribution. Pearson's Chi-Square test and Fisher-Freeman-Halton test were used for the comparisons of qualitative data.
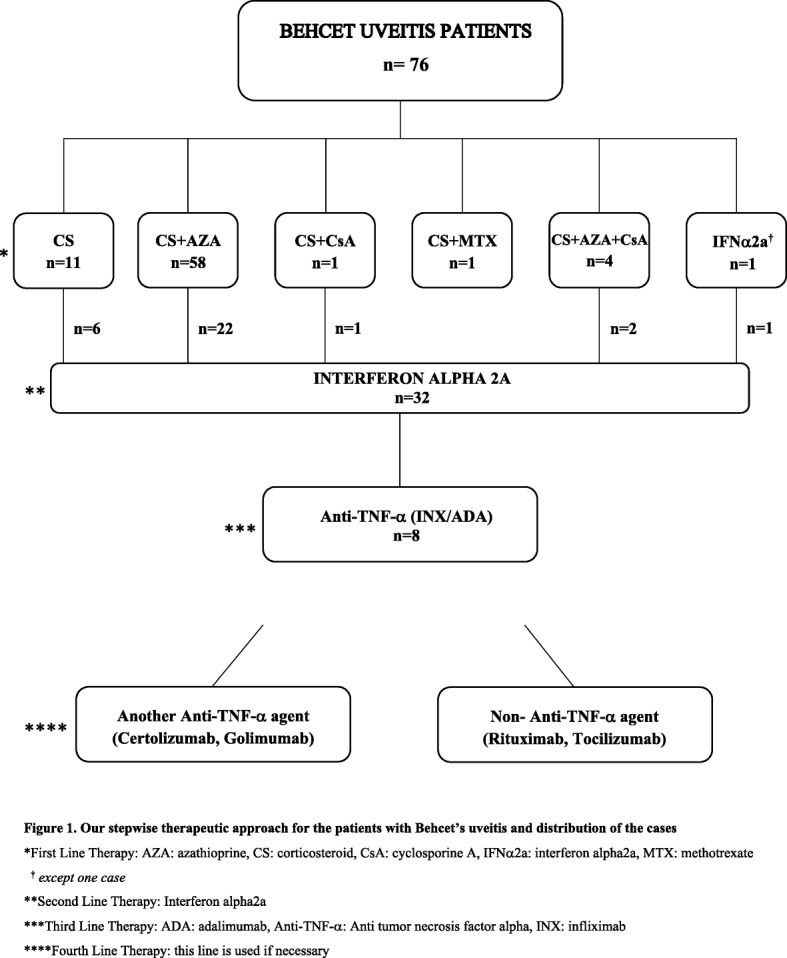
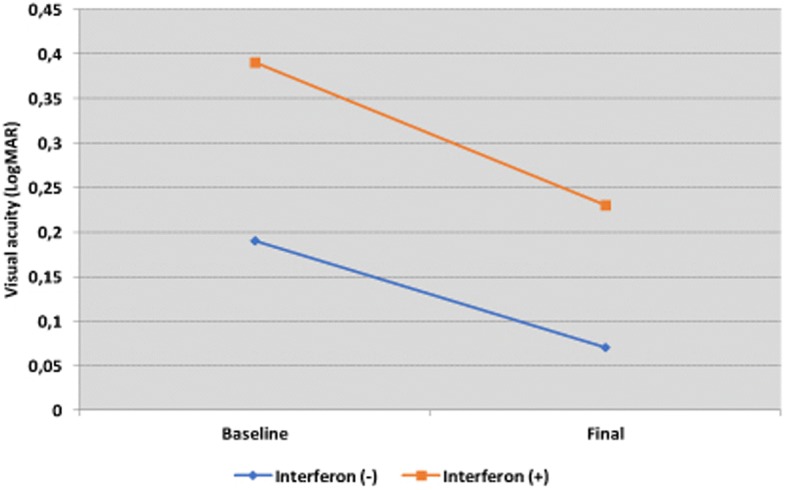
Results: Except for one, all patients were first treated with CIS regimens for BU. Thirty-one patients (41.3%) who were unresponsive to CIS regimens were switched to IFNα2a therapy. After that, eight of these cases were switched to the anti-TNF-α treatments. The presence of initial ocular complications were found to be statistically higher in BA treated patients than the CIS treated cases (p < 0.001). Both in CIS treated and in BA treated cases, an increase in visual acuity (VA) was observed during the last examination compared to the initial examination and was significant (p < 0.001 and p = 0.018, respectively).
Conclusions: CIS treatment was found to be effective and safe, as suggested in the management guidelines for severe BU. Biological therapy was also found effective for the improvement of the VA. We observed that 58.7% of cases could be treated with strong immunosuppressive therapies, however, nearly half of the patients could have lost their VA if BAs were not existent. During the treatment course of severe cases with BU, classical therapy stage must still be protected as the first-line therapy due to the their reasonable activity and safety.
Keywords: Anti-TNF-α therapy; Behçet’s uveitis; Immunosuppressive therapy; Interferon therapy; Uveitis.
Conflict of interest statement
Ethics approval and consent to participate
This study was conducted in accordance with the amendments of the Declaration of Helsinki. The retrospective study protocol was approved by the Marmara University Human Research Ethics Committee, and informed consent was obtained from all participants before the study began.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Behçet H. Über rezidivierende aphthöse durch ein virus verursachte Geschwüre am Mund, am Auge, und an den Genitalien. Dermatol Wochenschr. 1937;105:1152–1157.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
