

Concomitant inhaled corticosteroid use and the risk of pneumonia in COPD: a matched-subgroup post hoc analysis of the UPLIFT® trial
- PMID: 30290801
- PMCID: PMC6173940
- DOI: 10.1186/s12931-018-0874-0
Concomitant inhaled corticosteroid use and the risk of pneumonia in COPD: a matched-subgroup post hoc analysis of the UPLIFT® trial
Abstract
Background: Use of inhaled corticosteroids (ICS) increases the risk of pneumonia in chronic obstructive pulmonary disease (COPD), but the magnitude of risk with different ICS remains unclear.
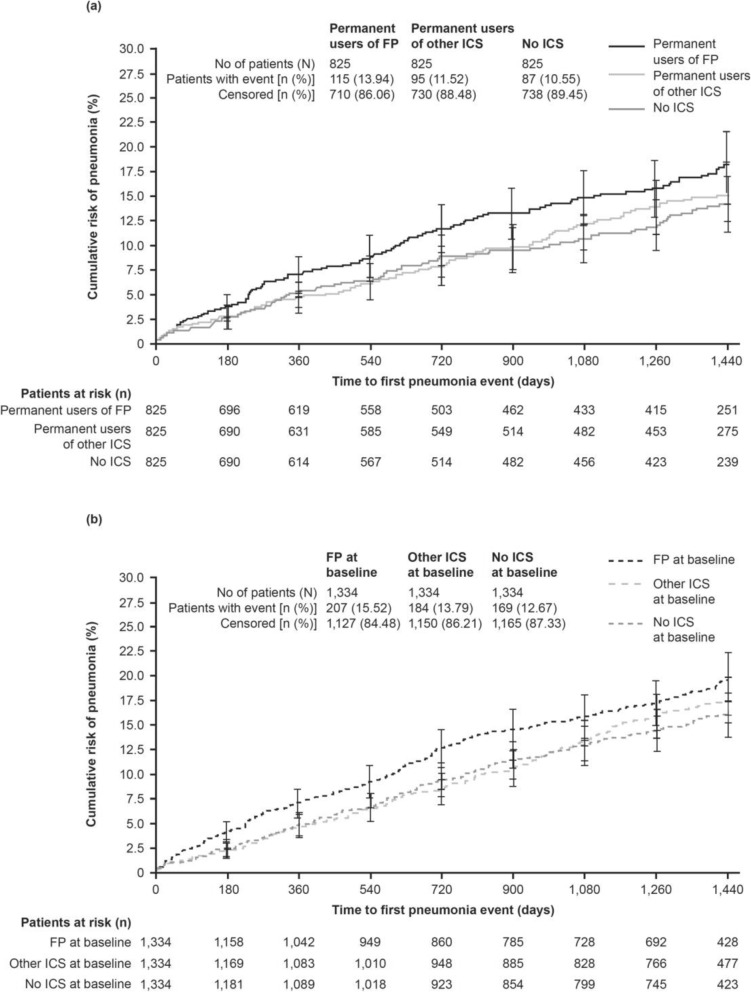
Methods: A post hoc analysis of the 4-year UPLIFT® trial to assess whether pneumonia risk differed by type of ICS (fluticasone propionate [FP], other ICS, or no ICS) in permanent users (defined by use until end of study) or in users at baseline (sensitivity analysis).
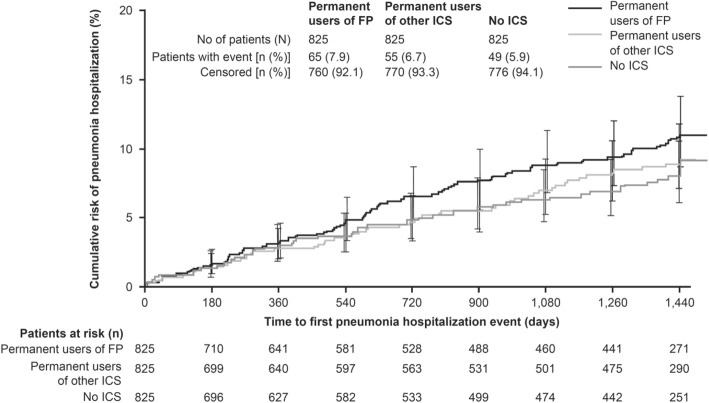
Results: For the permanent-users analysis, 825 patients receiving FP throughout the trial, 825 patients receiving other ICS and 825 patients not receiving ICS were matched on relevant baseline features 1:1:1. A significantly greater risk of pneumonia was observed for FP versus no ICS: the hazard ratio (HR) for risk of pneumonia was 1.33 (95% confidence interval [CI] 1.00, 1.75; p = 0.046) and the rate ratio (RR) was 1.58 (95% CI 1.05, 2.37; p = 0.028). A greater risk was also found for FP versus other ICS: HR 1.28 (95% CI 0.97, 1.68; p = 0.078) and RR 1.48 (95% CI 1.00, 2.19; p = 0.049). A higher proportion of patients on FP were hospitalized with pneumonia (7.9%) versus other ICS (6.7%) or no ICS (5.9%). Whilst other ICS use was associated with the highest number of fatal pneumonia events, the total number of fatal pneumonia incidents was low. A similar pattern was observed in the sensitivity analyses, which included 4002 patients on different treatments at baseline (FP, other ICS, and no ICS) and considered potential switches during the study.
Conclusion: The results support existing evidence of an increased pneumonia risk with FP use compared with other ICS and no ICS use in patients with COPD. Healthcare professionals should evaluate the risk-benefit ratio of using ICS when making treatment decisions with their patients.
Trial registration: Post hoc analysis of UPLIFT®. ClinicalTrials.gov number: NCT00144339 . Retrospectively registered September 2, 2005.
Keywords: COPD; Fluticasone propionate; Inhaled corticosteroids; Pneumonia; UPLIFT®.
Conflict of interest statement
Ethics approval and consent to participate
The UPLIFT® study was performed in accordance with the provisions of the Declaration of Helsinki (1996 version), in accordance with the International Conference on Harmonization Tripartite Guideline for Good Clinical Practice, and in accordance with applicable regulatory requirements and Boehringer Ingelheim Standard Operating Procedures. All patients provided written informed consent. This article does not report individual patient data; all data presented here is anonymized. The clinical trial protocol (dated 12 February 2002) and the informed consent and patient information forms were reviewed and received approval/favorable opinion from a constituted local Institutional Review Board or an Independent Ethics Committee at each center prior to the start of the study.
Competing interests
DPT has been an advisory board member and speaker for Boehringer Ingelheim, AstraZeneca and Sunovion; and a consultant for Mylan and Theravance/Innovative Pharmaceuticals. MM has received speaker fees from Boehringer Ingelheim, Chiesi, Cipla, Menarini, ROVI, Grifols and Novartis; and consulting fees from Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Gebro Pharma, CSL Behring, Novartis and Grifols. BRC has received consulting fees from Almirall, AstraZeneca, Boehringer Ingelheim and GlaxoSmithKline; lecture fees from Almirall, AstraZeneca, Boehringer Ingelheim and GlaxoSmithKline; and grant support from Boehringer Ingelheim, Forest Laboratories and GlaxoSmithKline. NM and AM are employees of Boehringer Ingelheim. DMGH has received personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Pfizer and Novartis. AA received grants or fees from AstraZeneca, Boehringer Ingelheim, Forest Laboratories, GlaxoSmithKline and Novartis.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- NICE National Clinical Guideline Centre. Chronic obstructive pulmonary disease in over 16s: diagnosis and management 2010.
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Am J Respir Crit Care Med. 2017;195:557–582. doi: 10.1164/rccm.201701-0218PP. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
