

Outcomes of a Digitally Delivered Low-Carbohydrate Type 2 Diabetes Self-Management Program: 1-Year Results of a Single-Arm Longitudinal Study
- PMID: 30291081
- PMCID: PMC6238840
- DOI: 10.2196/diabetes.9333
Outcomes of a Digitally Delivered Low-Carbohydrate Type 2 Diabetes Self-Management Program: 1-Year Results of a Single-Arm Longitudinal Study
Abstract
Background: Type 2 diabetes mellitus has serious health consequences, including blindness, amputation, stroke, and dementia, and its annual global costs are more than US $800 billion. Although typically considered a progressive, nonreversible disease, some researchers and clinicians now argue that type 2 diabetes may be effectively treated with a carbohydrate-reduced diet.
Objective: Our objective was to evaluate the 1-year outcomes of the digitally delivered Low-Carb Program, a nutritionally focused, 10-session educational intervention for glycemic control and weight loss for adults with type 2 diabetes. The program reinforces carbohydrate restriction using behavioral techniques including goal setting, peer support, and behavioral self-monitoring.
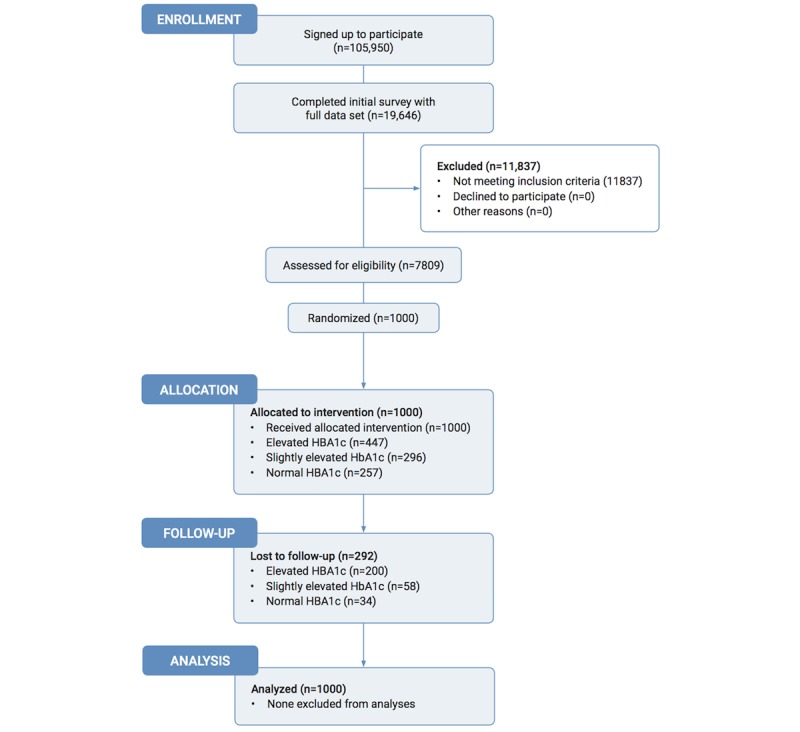
Methods: The study used a quasi-experimental research design comprised of an open-label, single-arm, pre-post intervention using a sample of convenience. From adults with type 2 diabetes who had joined the program and had a complete baseline dataset, we randomly selected participants to be followed for 1 year (N=1000; mean age 56.1, SD 15.7 years; 59.30% (593/1000) women; mean glycated hemoglobin A1c (HbA1c) 7.8%, SD 2.1%; mean body weight 89.6 kg, SD 23.1 kg; taking mean 1.2, SD 1.01 diabetes medications).
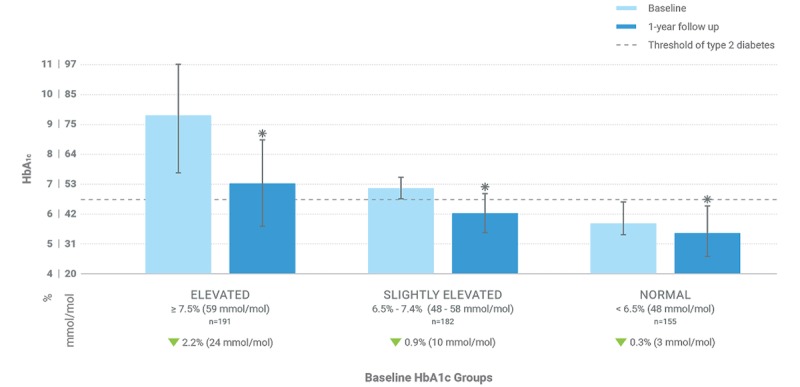
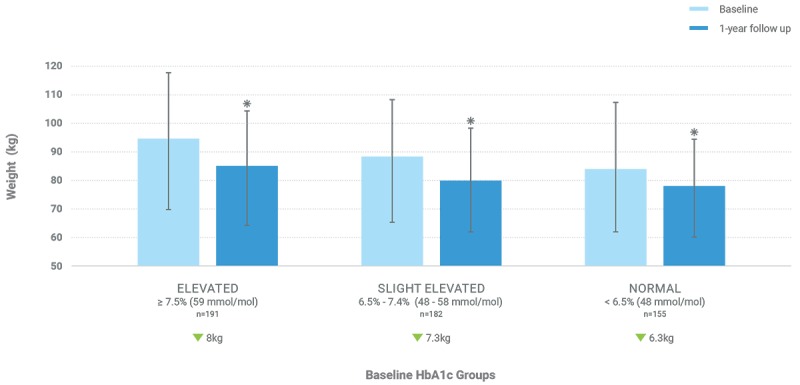
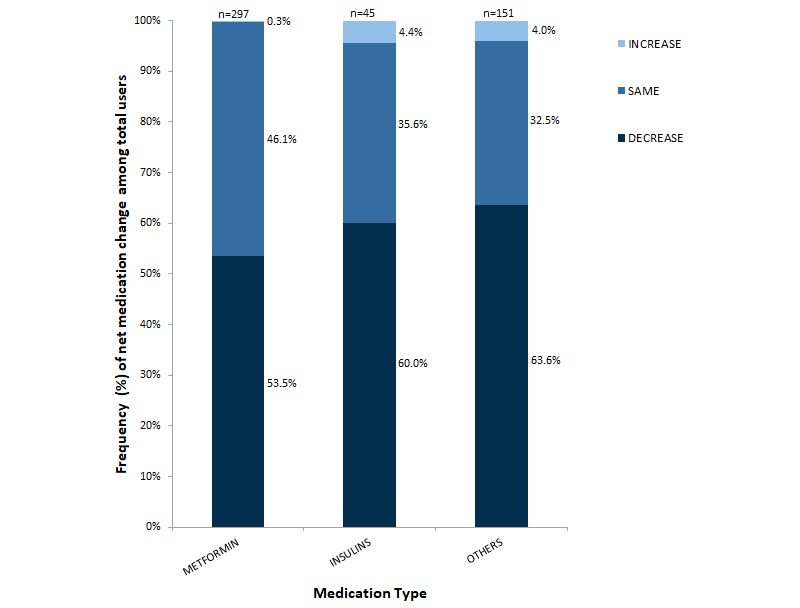
Results: Of the 1000 study participants, 708 (70.80%) individuals reported outcomes at 12 months, 672 (67.20%) completed at least 40% of the lessons, and 528 (52.80%) completed all lessons of the program. Of the 743 participants with a starting HbA1c at or above the type 2 diabetes threshold of 6.5%, 195 (26.2%) reduced their HbA1c to below the threshold while taking no glucose-lowering medications or just metformin. Of the participants who were taking at least one hypoglycemic medication at baseline, 40.4% (289/714) reduced one or more of these medications. Almost half (46.40%, 464/1000) of all participants lost at least 5% of their body weight. Overall, glycemic control and weight loss improved, especially for participants who completed all 10 modules of the program. For example, participants with elevated baseline HbA1c (≥7.5%) who engaged with all 10 weekly modules reduced their HbA1c from 9.2% to 7.1% (P<.001) and lost an average of 6.9% of their body weight (P<.001).
Conclusions: Especially for participants who fully engage, an online program that teaches a carbohydrate-reduced diet to adults with type 2 diabetes can be effective for glycemic control, weight loss, and reducing hypoglycemic medications.
Keywords: diet; eHealth; type 2 diabetes mellitus; weight loss.
©Laura R Saslow, Charlotte Summers, James E Aikens, David J Unwin. Originally published in JMIR Diabetes (http://diabetes.jmir.org), 03.08.2018.
Conflict of interest statement
Conflicts of Interest: CS is employed by Diabetes.co.uk, which runs the Low-Carb Program. The rest of the authors declare no conflicts of interest.
Figures
References
-
- Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D, Turner RC, Holman RR. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000 Aug 12;321(7258):405–412. http://europepmc.org/abstract/MED/10938048 - PMC - PubMed
-
- World Health Organization. 2016. [2018-04-15]. Global report on diabetes http://www.who.int/diabetes/global-report/en/
-
- Dieleman JL, Baral R, Birger M, Bui AL, Bulchis A, Chapin A, Hamavid H, Horst C, Johnson EK, Joseph J, Lavado R, Lomsadze L, Reynolds A, Squires E, Campbell M, DeCenso B, Dicker D, Flaxman AD, Gabert R, Highfill T, Naghavi M, Nightingale N, Templin T, Tobias MI, Vos T, Murray CJ. US spending on personal health care and public health, 1996-2013. JAMA. 2016 Dec 27;316(24):2627–2646. doi: 10.1001/jama.2016.16885. http://europepmc.org/abstract/MED/28027366 2594716 - DOI - PMC - PubMed
-
- Seuring T, Archangelidi O, Suhrcke M. The economic costs of type 2 diabetes: a global systematic review. Pharmacoeconomics. 2015 Aug;33(8):811–831. doi: 10.1007/s40273-015-0268-9. http://europepmc.org/abstract/MED/25787932 - DOI - PMC - PubMed
-
- Karter AJ, Nundy S, Parker MM, Moffet HH, Huang ES. Incidence of remission in adults with type 2 diabetes: the diabetes & aging study. Diabetes Care. 2014 Dec;37(12):3188–3195. doi: 10.2337/dc14-0874. http://europepmc.org/abstract/MED/25231895 dc14-0874 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
