

Screening for Adverse Drug Events: a Randomized Trial of Automated Calls Coupled with Phone-Based Pharmacist Counseling
- PMID: 30291602
- PMCID: PMC6374268
- DOI: 10.1007/s11606-018-4672-7
Screening for Adverse Drug Events: a Randomized Trial of Automated Calls Coupled with Phone-Based Pharmacist Counseling
Abstract
Background: Medication adverse events are important and common yet are often not identified by clinicians. We evaluated an automated telephone surveillance system coupled with transfer to a live pharmacist to screen potentially drug-related symptoms after newly starting medications for four common primary care conditions: hypertension, diabetes, depression, and insomnia.
Methods: Cluster randomized trial with automated calls to eligible patients at 1 and 4 months after starting target drugs from intervention primary care clinics compared to propensity-matched patients from control clinics. Primary and secondary outcomes were physician documentation of any adverse effects associated with newly prescribed target medication, and whether the medication was discontinued and, if yes, whether the reason for stopping was an adverse effect.
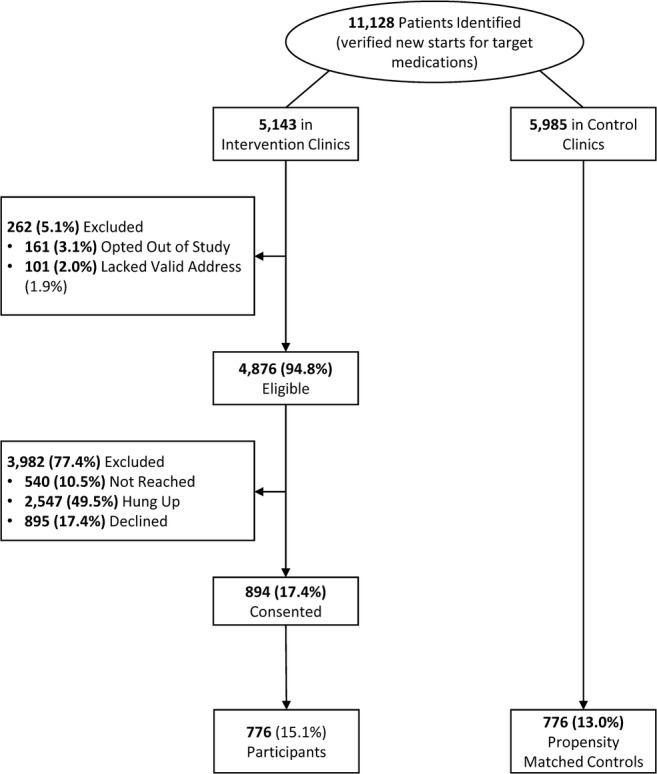
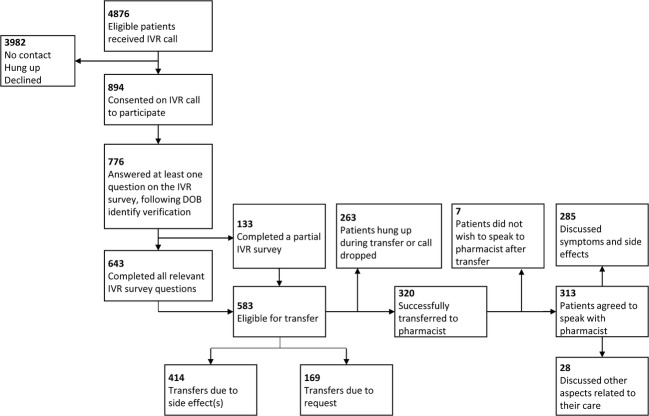
Results: Of 4876 eligible intervention clinic patients who were contacted using automated calls, 776 (15.1%) responded and participated in the automated call. Based on positive symptom responses or request to speak to a pharmacist, 320 patients were transferred to the pharmacist and discussed 1021 potentially drug-related symptoms. Of these, 188 (18.5%) were assessed as probably and 479 (47.1%) as possibly related to the medication. Compared to a propensity-matched cohort of control clinic patients, intervention patients were significantly more likely to have adverse effects documented in the medical record by a physician (277 vs. 164 adverse effects, p < 0.0001, and 177 vs. 122 patients discontinued with documented adverse effects, p < 0.0001).
Discussion: Systematic automated telephone outreach monitoring coupled with real-time phone referral to a pharmacist identified a substantial number of previously unidentified potentially drug-related symptoms, many of which were validated as probably or possibly related to the drug by the pharmacist or their physicians. Multiple challenges were encountered using the interactive voice response (IVR) automated calling system, suggesting that other approaches may need to be considered and evaluated.
Trial registration: ClinicalTrials.gov : NCT02087293.
Conflict of interest statement
Dr. Schiff previously received grant compensation to evaluate the Medaware software. Dr. Bates consults for EarlySense, which makes patient safety monitoring systems. He receives cash compensation from CDI (Negev), Ltd., which is a not-for-profit incubator for health IT startups. He receives equity from ValeraHealth which makes software to help patients with chronic diseases. He receives equity from Clew which makes software to support clinical decision-making in intensive care. He receives equity from MDClone which takes clinical data and produces deidentified versions of it. Dr. Schiff’s and Dr. Bates’ financial interests have been reviewed by Brigham and Women’s Hospital and Partners HealthCare in accordance with their institutional policies.
The remaining authors declare no potential conflicts of interest.
Figures
References
-
- CDC. National Center for Health Statistics: Therapeutic Drug Use. 2015; http://www.cdc.gov/nchs/fastats/drug-use-therapeutic.htm. Accessed 12/5/2016.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
