

Multiple introductions and subsequent transmission of multidrug-resistant Candida auris in the USA: a molecular epidemiological survey
- PMID: 30293877
- PMCID: PMC6556114
- DOI: 10.1016/S1473-3099(18)30597-8
Multiple introductions and subsequent transmission of multidrug-resistant Candida auris in the USA: a molecular epidemiological survey
Abstract
Background: Transmission of multidrug-resistant Candida auris infection has been reported in the USA. To better understand its emergence and transmission dynamics and to guide clinical and public health responses, we did a molecular epidemiological investigation of C auris cases in the USA.
Methods: In this molecular epidemiological survey, we used whole-genome sequencing to assess the genetic similarity between isolates collected from patients in ten US states (California, Connecticut, Florida, Illinois, Indiana, Maryland, Massachusetts, New Jersey, New York, and Oklahoma) and those identified in several other countries (Colombia, India, Japan, Pakistan, South Africa, South Korea, and Venezuela). We worked with state health departments, who provided us with isolates for sequencing. These isolates of C auris were collected during the normal course of clinical care (clinical cases) or as part of contact investigations or point prevalence surveys (screening cases). We integrated data from standardised case report forms and contact investigations, including travel history and epidemiological links (ie, patients that had shared a room or ward with a patient with C auris). Genetic diversity of C auris within a patient, a facility, and a state were evaluated by pairwise differences in single-nucleotide polymorphisms (SNPs).
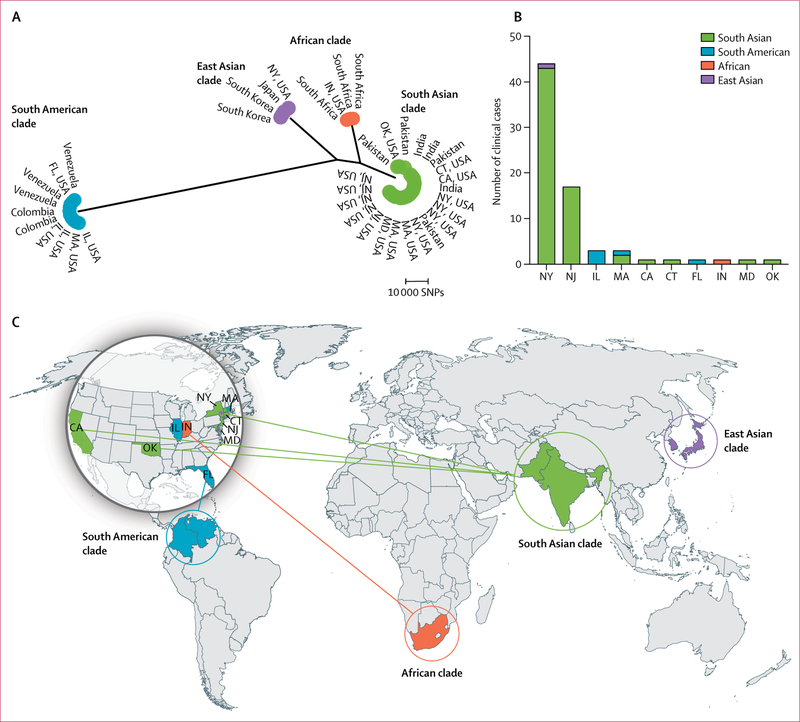
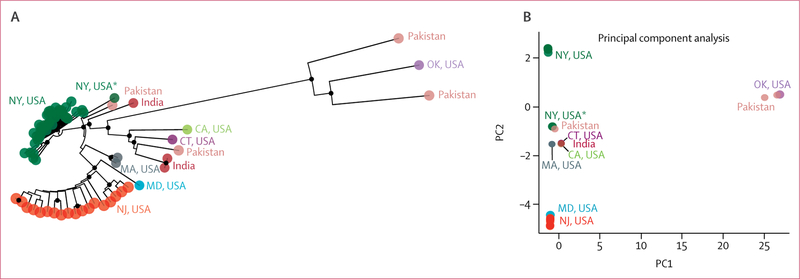
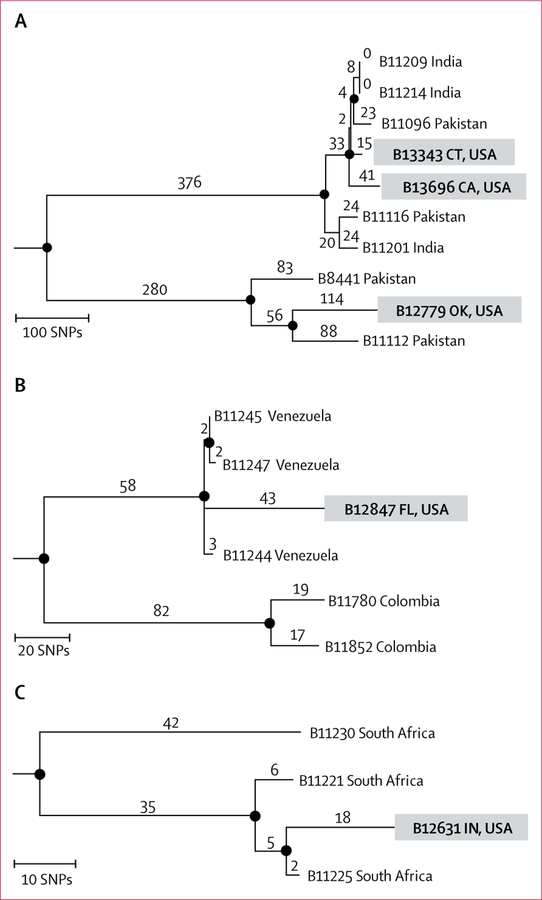
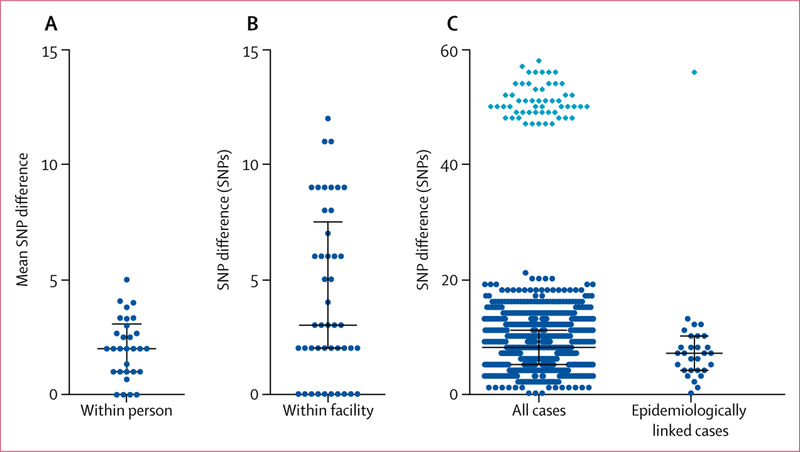
Findings: From May 11, 2013, to Aug 31, 2017, isolates that corresponded to 133 cases (73 clinical cases and 60 screening cases) were collected. Of 73 clinical cases, 66 (90%) cases involved isolates related to south Asian isolates, five (7%) cases were related to South American isolates, one (1%) case to African isolates, and one (1%) case to east Asian isolates. Most (60 [82%]) clinical cases were identified in New York and New Jersey; these isolates, although related to south Asian isolates, were genetically distinct. Genomic data corroborated five (7%) clinical cases in which patients probably acquired C auris through health-care exposures abroad. Among clinical and screening cases, the genetic diversity of C auris isolates within a person was similar to that within a facility during an outbreak (median SNP difference three SNPs, range 0-12).
Interpretation: Isolates of C auris in the USA were genetically related to those from four global regions, suggesting that C auris was introduced into the USA several times. The five travel-related cases are examples of how introductions can occur. Genetic diversity among isolates from the same patients, health-care facilities, and states indicates that there is local and ongoing transmission.
Funding: US Centers for Disease Control and Prevention.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
We declare no competing interests.
Figures
Comment in
-
Candida auris: a global fungal public health threat.Lancet Infect Dis. 2018 Dec;18(12):1298-1299. doi: 10.1016/S1473-3099(18)30609-1. Epub 2018 Oct 4. Lancet Infect Dis. 2018. PMID: 30293876 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
