

doi: 10.1093/eurheartj/ehy596.
Heart failure and diabetes: metabolic alterations and therapeutic interventions: a state-of-the-art review from the Translational Research Committee of the Heart Failure Association-European Society of Cardiology
Affiliations
- PMID: 30295797
- PMCID: PMC6302261
- DOI: 10.1093/eurheartj/ehy596
Item in Clipboard
Heart failure and diabetes: metabolic alterations and therapeutic interventions: a state-of-the-art review from the Translational Research Committee of the Heart Failure Association-European Society of Cardiology
Eur Heart J.
.
No abstract available
Figures

Systemic interdependence of heart failure and type 2 diabetes mellitus. In heart failure, neuroendocrine activation alters haemodynamics and metabolism, predisposing to the development of diabetes through insulin resistance. In diabetes, hyperglycaemia induces macro- and microvascular dysfunction, and myocardial ischaemia and/or infarction bias towards systolic dysfunction (heart failure with reduced ejection fraction), while in the absence of ischaemia, diastolic dysfunction (heart failure with preserved ejection fraction) prevails through a combination of sarcomere stiffness and fibrosis. Inflammation is a key systemic factor that contributes to several of these processes. The specific points of intervention by glucose-lowering drugs are indicated (all have in common that they lowed hyperglycaemia). AGEs, advanced glycation end products; AMP, adenosine monophosphate; AMPK, AMP-kinase; DPP4/GLP1, DPP4-inhibitors/GLP-1 analogons; SGLT2, SGLT2-inhibitors.

Cardiac metabolic alterations in heart failure. In heart failure, increased uptake of free fatty acids and glucose into the cytosol is uncoupled from mitochondrial uptake and oxidation of free fatty acid and pyruvate, respectively. This provokes accumulation of metabolic intermediates in the cytosol which can trigger lipo- and glucotoxicity. Instead, utilization of ketone bodies is increased in heart failure. Impaired overall substrate oxidation reduces Krebs cycle (TCA) activity, oxidizing electron donors NADH and FADH2 for the electron transport chain (ETC). This reduces metabolic flux through creatine kinase (CK), thereby the phosphocreatine (PCr) to ATP ratio. β-Ox., β-oxidation; CPT-1/2, carnitine palmitoyltransferase type 1/2; FA-CoA, fatty acyl-coenzyme A; FACS, fatty acyl-coenzyme A synthetase; FAT/CD36, fatty acid translocase; GLUT 1/4, glucose transporters 1/4; G6P, glucose-6-phosphate; PDH, pyruvate dehydrogenase complex; PPP, pentose phosphate pathway; Polyol P., Polyol pathway; TAG, triacylglycerol; UDPGlcNac, UDP-glycnacylation. Red arrows (↓↑) indicate the changes in heart failure.

Cardiac metabolic alterations in diabetes. In diabetes, strongly increased free fatty acid activate peroxisome proliferator-activated receptor α (PPARα), which up-regulates expression of genes involved in fatty acid (FA) oxidation. Increased FA oxidation shuts down glucose uptake and oxidation (insulin resistance), thereby blunts metabolic flexibility. Excessive FA are stored as triacylglycerol (TAG), which can mediate lipotoxicity. FA and reactive oxygen species (ROS) activate uncoupling protein 3 (UCP3), which makes ATP production less efficient. Abbreviations see legend of Figure 2.

Metabolic interventions in diabetes and heart failure. For details see text. DPP4/GLP1, DPP4-inhibitors/GLP-1 analogons; SGLT2, SGLT2-inhibitors.
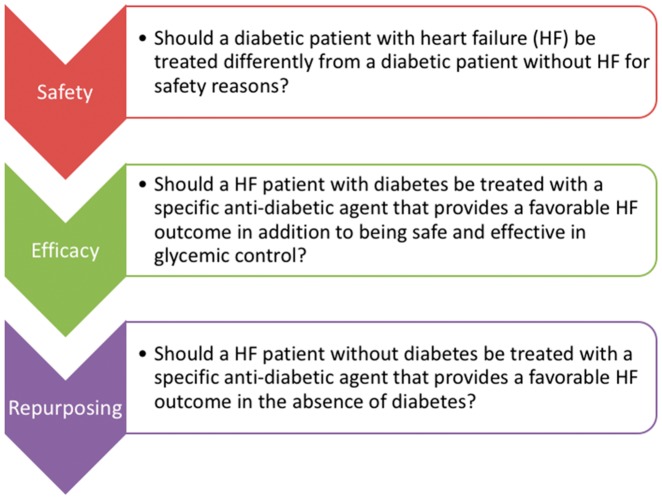
Basic concepts concerning the use of anti-diabetic drugs in patients with heart failure.
Comment in
-
The possible role of insulin and glucagon in patients with heart failure and Type 2 diabetes.Eur Heart J. 2020 Jan 7;41(2):325. doi: 10.1093/eurheartj/ehz242. Eur Heart J. 2020. PMID: 31323668 No abstract available.
-
Response to 'The possible role of insulin and glucagon in patients with heart failure and Type 2 diabetes'.Eur Heart J. 2020 Jan 7;41(2):326-327. doi: 10.1093/eurheartj/ehz243. Eur Heart J. 2020. PMID: 31329851 No abstract available.
References
-
- Farmakis D, Stafylas P, Giamouzis G, Maniadakis N, Parissis J.. The medical and socioeconomic burden of heart failure: a comparative delineation with cancer. Int J Cardiol 2016;203:279–281. - PubMed
-
- Voors AA, van Veldhuisen DJ.. Why do drugs for acute heart failure fail? Eur J Heart Fail 2012;14:955–956. - PubMed
-
- Lombardi C, Spigoni V, Gorga E, Dei Cas A.. Novel insight into the dangerous connection between diabetes and heart failure. Herz 2016;41:201–207. - PubMed
-
- Paulus WJ, Tschope C.. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol 2013;62:263–271. - PubMed
