

Drug Targets for Heart Failure with Preserved Ejection Fraction: A Mechanistic Approach and Review of Contemporary Clinical Trials
- PMID: 30296895
- PMCID: PMC6327844
- DOI: 10.1146/annurev-pharmtox-010818-021136
Drug Targets for Heart Failure with Preserved Ejection Fraction: A Mechanistic Approach and Review of Contemporary Clinical Trials
Abstract
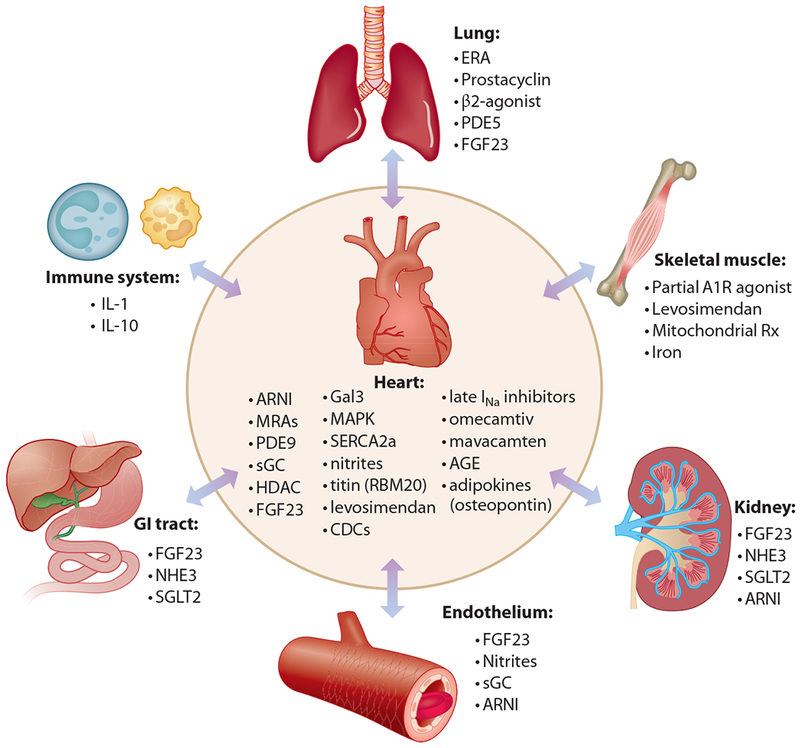
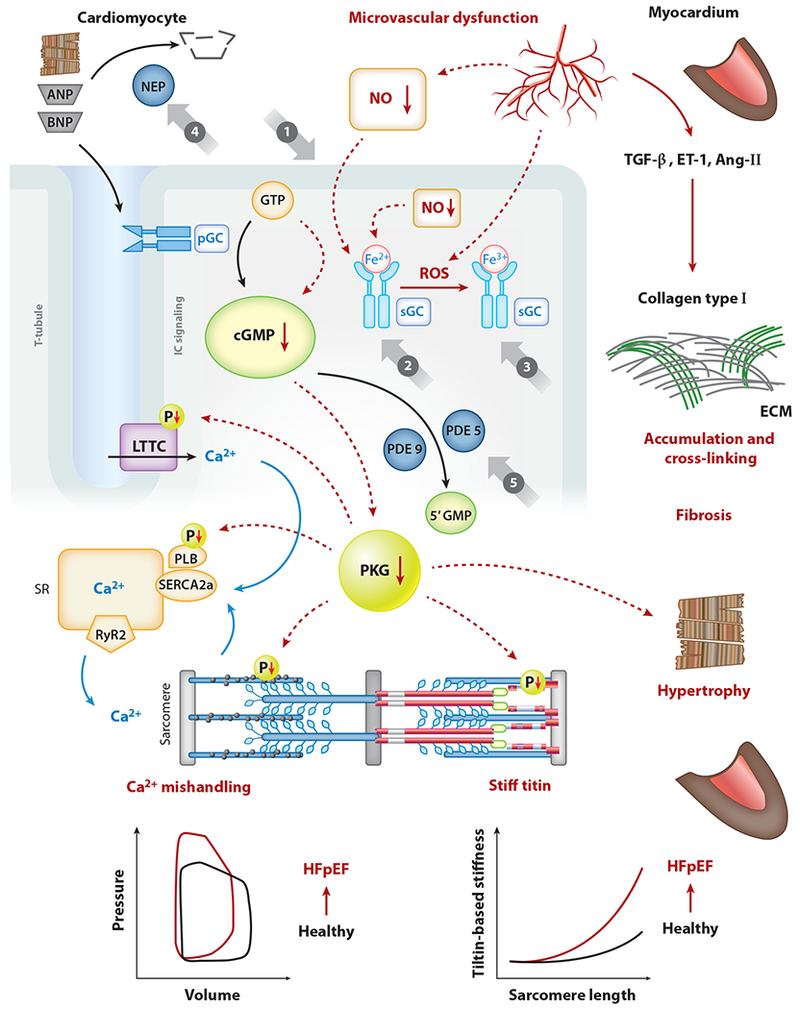
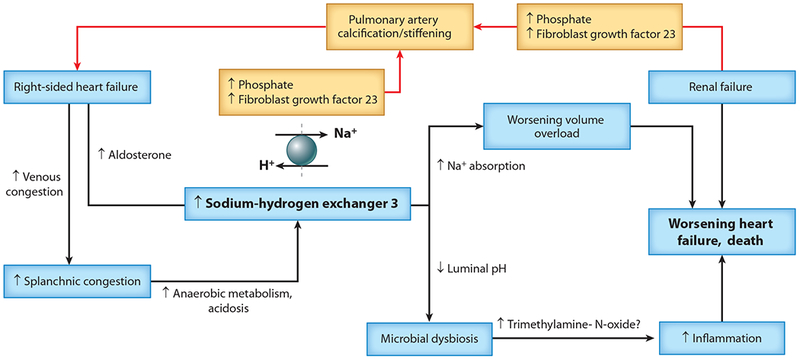
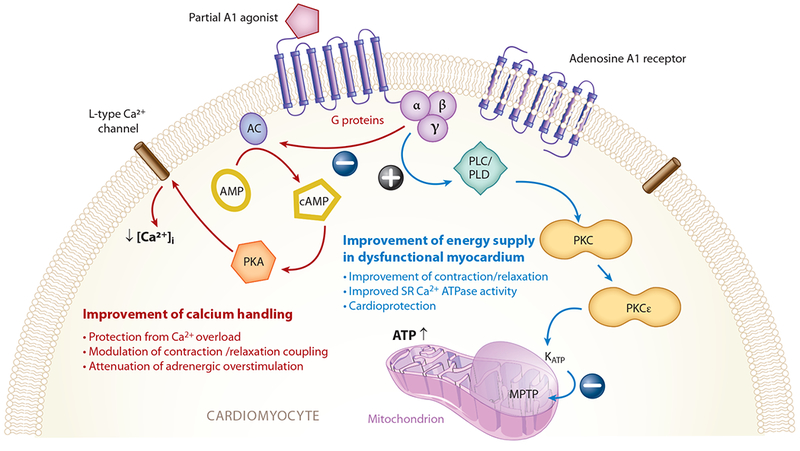
Heart failure with preserved ejection fraction (HFpEF) accounts for over half of prevalent heart failure (HF) worldwide, and prognosis after hospitalization for HFpEF remains poor. Due, at least in part, to the heterogeneous nature of HFpEF, drug development has proved immensely challenging. Currently, there are no universally accepted therapies that alter the clinical course of HFpEF. Despite these challenges, important mechanistic understandings of the disease have revealed that the pathophysiology of HFpEF is distinct from that of HF with reduced ejection fraction and have also highlighted potential new therapeutic targets for HFpEF. Of note, HFpEF is a systemic syndrome affecting multiple organ systems. Depending on the organ systems involved, certain novel therapies offer promise in reducing the morbidity of the HFpEF syndrome. In this review, we aim to discuss novel pharmacotherapies for HFpEF based on its unique pathophysiology and identify key research strategies to further elucidate mechanistic pathways to develop novel therapeutics in the future.
Keywords: heart failure with preserved ejection fraction; pathophysiology; pharmacotherapy.
Figures
References
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, et al. 2014. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol 63:1123–33 - PubMed
-
- Vaduganathan M, Michel A, Hall K, Mulligan C, Nodari S, et al. 2016. Spectrum of epidemiological and clinical findings in patients with heart failure with preserved ejection fraction stratified by study design: a systematic review. Eur. J. Heart Fail 18:54–65 - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. 2006. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N. Engl. J. Med 355:251–59 - PubMed
-
- Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, et al. 2008. Irbesartan in patients with heart failure and preserved ejection fraction. N. Engl. J. Med 359:2456–67 - PubMed
-
- Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, et al. 2014. Spironolactone for heart failure with preserved ejection fraction. N. Engl. J. Med 370:1383–92 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
