

Effect of in utero hydroxychloroquine exposure on the development of cutaneous neonatal lupus erythematosus
- PMID: 30297329
- PMCID: PMC6382275
- DOI: 10.1136/annrheumdis-2018-213718
Effect of in utero hydroxychloroquine exposure on the development of cutaneous neonatal lupus erythematosus
Abstract
Objective: Cutaneous neonatal lupus (cNL) occurs in possibly 5%-16% of anti-Ro±anti-La antibody-exposed infants. Data suggest in utero exposure to hydroxychloroquine (HCQ) may prevent cardiac NL. The aim was to assess whether in utero exposure to HCQ decreases the risk of cNL and/or delays onset.
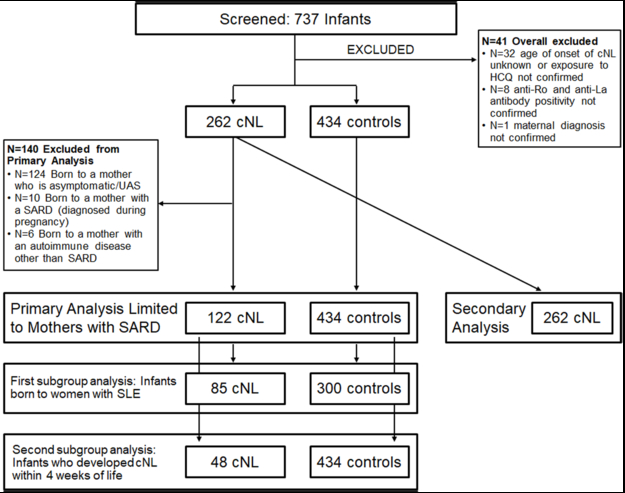
Methods: A multicentre case-control study was performed with 122 cNL cases and 434 controls born to women with a rheumatological disease who had documentation of maternal anti-Ro±anti-La antibodies at pregnancy and confirmation of medication use and the child's outcome. A secondary analysis was performed on 262 cNL cases, irrespective of maternal diagnosis, to determine if HCQ delayed time to cNL onset.
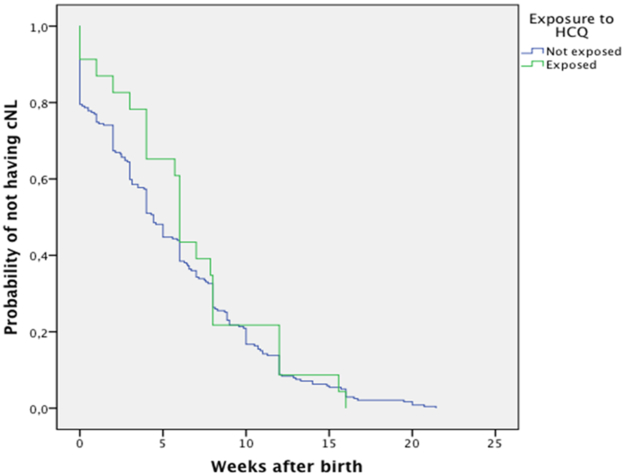
Results: Twenty (16%) cNL cases were exposed to HCQ compared with 146 (34%) controls (OR 0.4 (95% CI 0.2 to 0.6); p<0.01). Exposure to HCQ was associated with a reduced risk of cNL; exposure to anti-La antibody and female gender were associated with an increased risk of cNL. Exposure to HCQ remained significantly associated with a reduced cNL risk in the analyses limited to mothers with systemic lupus erythematosus and those who developed rash ≤1 month. When analysing all 262 cNL cases, HCQ-exposed infants were older (6.0 (95% CI 5.7 to 6.3) weeks) at cNL onset versus HCQ-non-exposed infants (4.4 (95% CI 3.9 to 5.0) weeks), but the difference was not statistically significant (p=0.21).
Conclusion: Exposure to HCQ was associated with a reduced risk of cNL. Among cNL cases, those exposed to HCQ tend to have later onset of rash. Both findings suggest a protective effect of HCQ on cNL.
Keywords: Sjøgren's syndrome; systemic lupus erythematosus; treatment.
© Author(s) (or their employer(s)) 2018. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Cimaz R, Spence DL, Hornberger L et al. Incidence and spectrum of neonatal lupus erythematosus: a prospective study of infants born to mothers with anti-Ro autoantibodies. J Pediatr 2003;142(6):678–83. - PubMed
-
- Friedman DM, Kim MY, Copel JA, et al. Utility of cardiac monitoring in fetuses at risk for congenital heart block: the PR Interval and Dexamethasone Evaluation (PRIDE) prospective study. Circulation 2008;117(4):485–93. - PubMed
-
- Penate Y, Guillermo N, Rodriguez J, et al. Histopathologic characteristics of neonatal cutaneous lupus erythematosus: description of five cases and literature review. J Cutan Pathol 2009;36(6):660–7. - PubMed
-
- Neiman AR, Lee LA, Weston WL et al. Cutaneous manifestations of neonatal lupus without heart block: characteristics of mothers and children enrolled in a national registry. J Pediatr 2000;137(5):674–80. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
