

Laparoscopic cholecystectomy versus percutaneous catheter drainage for acute cholecystitis in high risk patients (CHOCOLATE): multicentre randomised clinical trial
- PMID: 30297544
- PMCID: PMC6174331
- DOI: 10.1136/bmj.k3965
Laparoscopic cholecystectomy versus percutaneous catheter drainage for acute cholecystitis in high risk patients (CHOCOLATE): multicentre randomised clinical trial
Abstract
Objective: To assess whether laparoscopic cholecystectomy is superior to percutaneous catheter drainage in high risk patients with acute calculous cholecystitis.
Design: Multicentre, randomised controlled, superiority trial.
Setting: 11 hospitals in the Netherlands, February 2011 to January 2016.
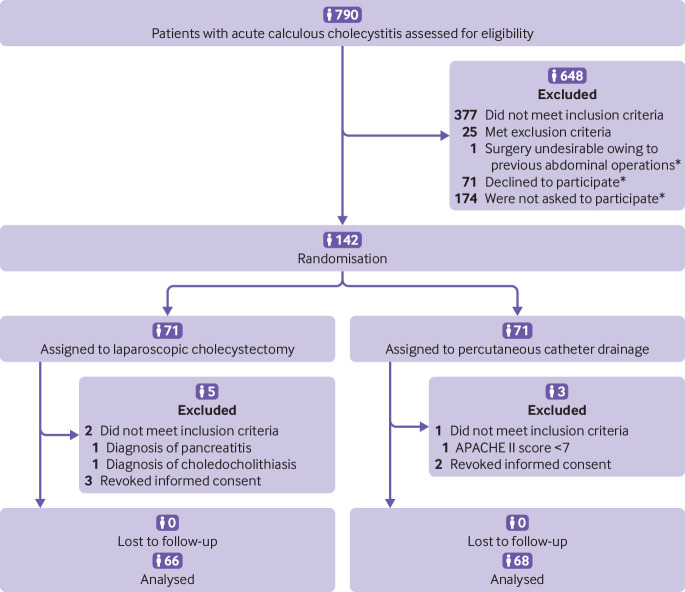
Participants: 142 high risk patients with acute calculous cholecystitis were randomly allocated to laparoscopic cholecystectomy (n=66) or to percutaneous catheter drainage (n=68). High risk was defined as an acute physiological assessment and chronic health evaluation II (APACHE II) score of 7 or more.
Main outcome measures: The primary endpoints were death within one year and the occurrence of major complications, defined as infectious and cardiopulmonary complications within one month, need for reintervention (surgical, radiological, or endoscopic that had to be related to acute cholecystitis) within one year, or recurrent biliary disease within one year.
Results: The trial was concluded early after a planned interim analysis. The rate of death did not differ between the laparoscopic cholecystectomy and percutaneous catheter drainage group (3% v 9%, P=0.27), but major complications occurred in eight of 66 patients (12%) assigned to cholecystectomy and in 44 of 68 patients (65%) assigned to percutaneous drainage (risk ratio 0.19, 95% confidence interval 0.10 to 0.37; P<0.001). In the drainage group 45 patients (66%) required a reintervention compared with eight patients (12%) in the cholecystectomy group (P<0.001). Recurrent biliary disease occurred more often in the percutaneous drainage group (53% v 5%, P<0.001), and the median length of hospital stay was longer (9 days v 5 days, P<0.001).
Conclusion: Laparoscopic cholecystectomy compared with percutaneous catheter drainage reduced the rate of major complications in high risk patients with acute cholecystitis.
Trial registration: Dutch Trial Register NTR2666.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf declare no support from any organisation for the submitted work, no financial relationships with any organizations that might have an interest in the submitted work, and no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Cholecystectomy reduced major complications vs catheter drainage in high-risk patients with acute cholecystitis.Ann Intern Med. 2019 Feb 19;170(4):JC22. doi: 10.7326/ACPJ201902190-022. Ann Intern Med. 2019. PMID: 30776811 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical