

European headache federation guideline on idiopathic intracranial hypertension
- PMID: 30298346
- PMCID: PMC6755569
- DOI: 10.1186/s10194-018-0919-2
European headache federation guideline on idiopathic intracranial hypertension
Abstract
Background: Idiopathic Intracranial Hypertension (IIH) is characterized by an elevation of intracranial pressure (ICP no identifiable cause. The aetiology remains largely unknown, however observations made in a number of recent clinical studies are increasing the understanding of the disease and now provide the basis for evidence-based treatment strategies.
Methods: The Embase, CDSR, CENTRAL, DARE and MEDLINE databases were searched up to 1st June 2018. We analyzed randomized controlled trials and systematic reviews that investigate IIH.
Results: Diagnostic uncertainty, headache morbidity and visual loss are among the highest concerns of clinicians and patients in this disease area. Research in this field is infrequent due to the rarity of the disease and the lack of understanding of the underlying pathology.
Conclusions: This European Headache Federation consensus paper provides evidence-based recommendations and practical advice on the investigation and management of IIH.
Conflict of interest statement
JH received honoraria for consulting for and/or serving on advisory boards for Allergan, Autonomic Technologies Inc. (ATI), Chordate Medical AB, Eli Lilly, Hormosan Pharma, Novartis and Teva. He received honoraria for speaking from Allergan, Autonomic Technologies Inc. (ATI), Chordate Medical AB, Novartis and Teva. These activities are/were unrelated to the submitted work. SPM reports no conflict of interest. KP reports no conflict of interest. CL reports no conflict of interest. RHJ has received honoraria for lectures and patient leaflets from MSD, Berlin-Chemie, Menarini, Autonomic Technologies Inc. (ATI) and Pfizer; participated in medical advisory boards for ATI and Electrocore and conducted clinical trials for ATI and Eli Lilly. AJS reports no conflict of interest.
Figures
Similar articles
-
Idiopathic intracranial hypertension.Neurol Clin. 2010 Aug;28(3):593-617. doi: 10.1016/j.ncl.2010.03.003. Neurol Clin. 2010. PMID: 20637991 Free PMC article.
-
Headache attributed to idiopathic intracranial hypertension and persistent post-idiopathic intracranial hypertension headache: A narrative review.Headache. 2021 Jun;61(6):808-816. doi: 10.1111/head.14125. Epub 2021 Jun 9. Headache. 2021. PMID: 34106464 Review.
-
The Pseudotumor Cerebri Syndrome.Neurol Clin. 2024 May;42(2):433-471. doi: 10.1016/j.ncl.2024.02.001. Neurol Clin. 2024. PMID: 38575259 Review.
-
What is new about idiopathic intracranial hypertension? An updated review of mechanism and treatment.Cephalalgia. 2006 Apr;26(4):384-99. doi: 10.1111/j.1468-2982.2005.01055.x. Cephalalgia. 2006. PMID: 16556239 Review.
-
[The diagnosis and management of idiopathic intracranial hypertension].Rev Med Suisse. 2021 Sep 8;17(749):1499-1505. Rev Med Suisse. 2021. PMID: 34495585 Review. French.
Cited by
-
Chiari Malformation Type 1 in Adults.Adv Tech Stand Neurosurg. 2023;46:149-173. doi: 10.1007/978-3-031-28202-7_8. Adv Tech Stand Neurosurg. 2023. PMID: 37318574
-
Investigation of Cranial Bone Changes Indicative of Increased Intracranial Pressure in Diverse Phenotypes of Craniosynostosis.Plast Reconstr Surg Glob Open. 2025 Mar 20;13(3):e6618. doi: 10.1097/GOX.0000000000006618. eCollection 2025 Mar. Plast Reconstr Surg Glob Open. 2025. PMID: 40115040 Free PMC article.
-
Management of idiopathic intracranial hypertension in pregnancy.Obstet Med. 2022 Sep;15(3):160-167. doi: 10.1177/1753495X211021333. Epub 2021 Jun 9. Obstet Med. 2022. PMID: 36262821 Free PMC article. Review.
-
What should otolaryngologists know about dural venous sinus stenting?Eur Arch Otorhinolaryngol. 2024 Nov;281(11):5619-5625. doi: 10.1007/s00405-024-08806-7. Epub 2024 Jul 23. Eur Arch Otorhinolaryngol. 2024. PMID: 39042170 Review.
-
Cerebrospinal Fluid Rhinorrhea Secondary to Idiopathic Intracranial Hypertension.Case Rep Neurol. 2019 Nov 14;11(3):295-298. doi: 10.1159/000503813. eCollection 2019 Sep-Dec. Case Rep Neurol. 2019. PMID: 31824283 Free PMC article.
References
-
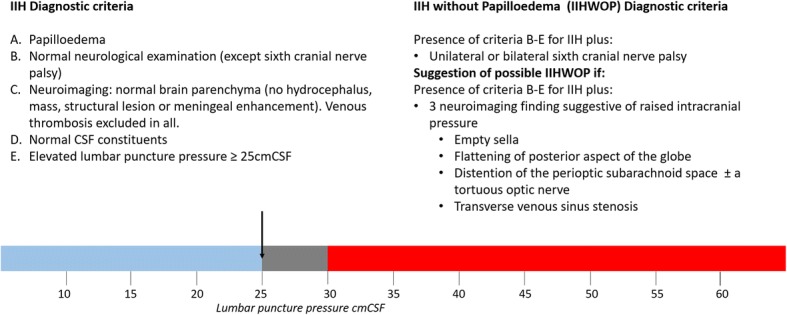
- Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2013;81(13):1159–1165. - PubMed
-
- Headache Classification Committee of the International Headache Society The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. - PubMed
-
- Markey KA, et al. Understanding idiopathic intracranial hypertension: mechanisms, management, and future directions. The Lancet Neurology. 2016;15(1):78–91. - PubMed
-
- Hoffmann J, Goadsby PJ. Update on intracranial hypertension and hypotension. Curr Opin Neurol. 2013;26(3):240–247. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
