

Impact of an HIV Care Coordination Program on Durable Viral Suppression
- PMID: 30299346
- PMCID: PMC6289598
- DOI: 10.1097/QAI.0000000000001877
Impact of an HIV Care Coordination Program on Durable Viral Suppression
Abstract
Background: To assess long-term effectiveness of an intensive and comprehensive Ryan White Part A-funded HIV Care Coordination Program recruiting people living with HIV with a history of suboptimal HIV care outcomes.
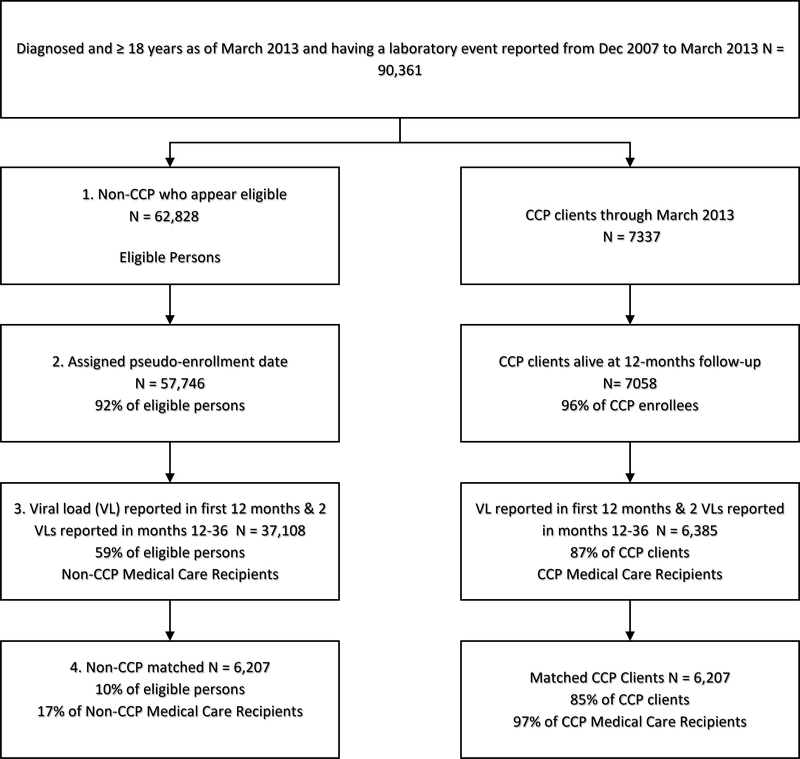
Methods: We merged programmatic data on CCP clients with surveillance data on all adults diagnosed with HIV. Using propensity score matching, we identified a contemporaneous, non-CCP-exposed comparison group. Durable viral suppression (DVS) was defined as regular viral load (VL) monitoring and all VLs ≤200 copies per milliliter in months 13-36 of follow-up.
Results: Ninety percent of the combined cohort (N = 12,414) had ≥1 VL ≤200 during the follow-up period (December 1, 2009-March 31, 2016), and nearly all had routine VL monitoring, but only 36.8% had DVS. Although DVS did not differ overall (relative risk: 0.99, 95% confidence interval: 0.95 to 1.03), CCP clients without any VL suppression (VLS) in the 12-month pre-enrollment showed higher DVS versus "usual care" recipients (21.3% versus 18.4%; relative risk: 1.16, 95% confidence interval: 1.04 to 1.29).
Conclusions: Enrollment in an intensive intervention modestly improved DVS among those unsuppressed before CCP enrollment. This program shows promise for meeting treatment-as-prevention goals and advancing progress along the HIV care continuum, if people without evidence of VLS are prioritized for CCP enrollment over those with recent evidence of VLS. Low overall DVS (<40%) levels underscore a need for focused adherence maintenance interventions, in a context of high treatment access.
Conflict of interest statement
Figures
References
-
- Temprano Anrs Study Group, Danel C, Moh R, et al. A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa. N Engl J Med. 2015;373(9):808–822. - PubMed
-
- Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet. 2009;373(9657):48–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
