

2018 Frank Stinchfield Award: Spinopelvic Hypermobility Is Associated With an Inferior Outcome After THA: Examining the Effect of Spinal Arthrodesis
- PMID: 30300162
- PMCID: PMC6370094
- DOI: 10.1097/CORR.0000000000000367
2018 Frank Stinchfield Award: Spinopelvic Hypermobility Is Associated With an Inferior Outcome After THA: Examining the Effect of Spinal Arthrodesis
Abstract
Background: Many patients undergo both THA and spinal arthrodesis, and those patients may not fare as well as those who undergo one procedure but not the other. The mechanisms of how spinal arthrodesis affects patient function after THA remain unclear.
Questions/purposes: The aims of our study were to (1) determine how patient-reported outcome measures (PROMs), including the Oxford hip score as well as dislocations and complications compare after THA between patients with and without spinal arthrodesis; (2) characterize sagittal pelvic changes in these patients that occur when moving between different functional positions and test for differences between patients with and without spinal arthrodesis; and (3) assess whether differences in sagittal pelvic dynamics are associated with PROMs, complications, and dislocations after THA.
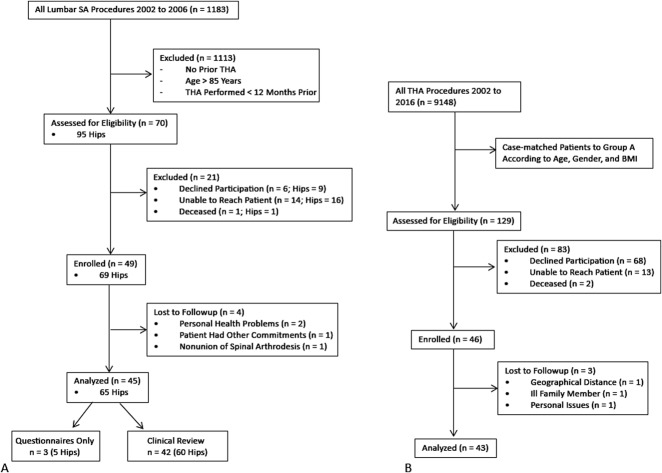
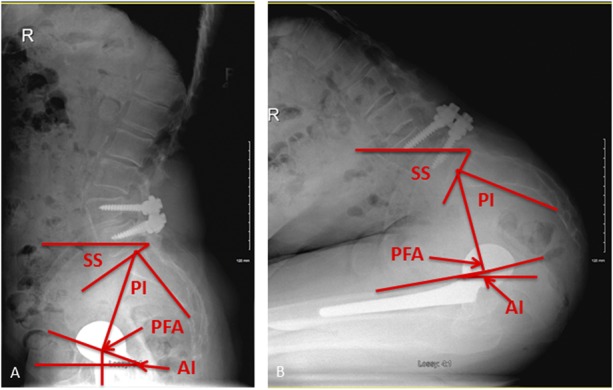
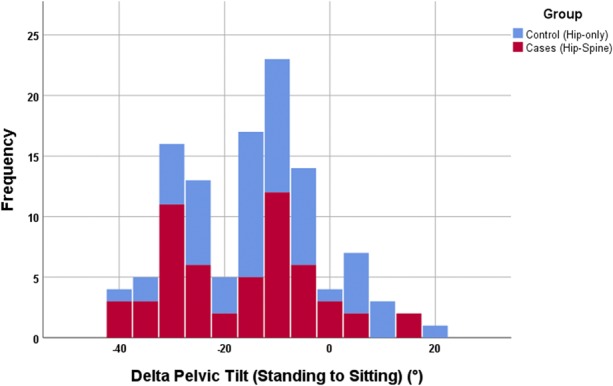
Methods: In this case-control study, we identified 42 patients (60 hips) who had undergone both THA and spinal arthrodesis between 2002 and 2016 and who were available for followup at a minimum of 12 months (mean, 6 ± 5 years) after the later of the two procedures. These cases were case-control-matched for age, gender, and body mass index with 42 patients (60 hips) who underwent only THA and had no known spinal pathology. All patients completed PROMs, including the Oxford hip score, and underwent four radiographs of the pelvis and spinopelvic complex in three positions (supine, standing, and deep-seated). Cup orientation and various spinopelvic parameters, including pelvic tilt and pelvic-femoral angle, were measured. The difference in pelvic tilt between standing and seated allowed for patient classification based on spinopelvic mobility into normal (± 10°-30°), stiff (< ± 10°) or hypermobile (> ± 30°) groups.
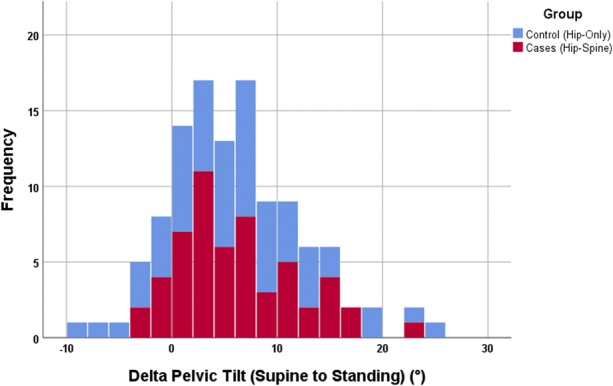
Results: Compared with the THA-only group, the THA-spinal arthrodesis group had inferior PROMs (Oxford hip score, 33 ± 10 versus 43 ± 6; p < 0.001) and more surgery-related complications (such as dislocation, loosening, periprosthetic fracture or infection, psoas irritation) (12 versus 3; p = 0.013), especially dislocation (5 versus 0; p = 0.023). We detected no difference in change of pelvic tilt between supine and standing positions between the groups. When standing, patients undergoing THA-spinal arthrodesis had greater pelvic tilt (25° ± 11° versus 17° ± 8°; p < 0.001) and the hip was more extended (193° ± 22° versus 185° ± 30°; p = 0.012). We found that patients undergoing THA-spinal arthrodesis were more likely to have spinopelvic hypermobility (12 of 42 versus three of 42; odds ratio, 5.2; p = 0.02) with anterior tilting of the pelvis. Of all biomechanical parameters, only spinopelvic hypermobility was associated with inferior PROMs (Oxford hip score, 35 ± 9 versus 40 ± 7 in normal mobility; p = 0.049) and was also present in dislocating hips that underwent revision despite acceptable cup orientation.
Conclusions: In patients with spinal arthrodesis who have undergone THA, spinopelvic hypermobility is associated with inferior outcomes, including hip instability. Spinopelvic hypermobility should be routinely assessed because these patients may have a narrow zone of optimum cup orientation that would require new technology to define and assist the surgeon in obtaining it.Level of Evidence Level III, therapeutic study.
Conflict of interest statement
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: 2018 Frank Stinchfield Award: Spinopelvic Hypermobility Is Associated With an Inferior Outcome After THA: Examining the Effect of Spinal Arthrodesis.Clin Orthop Relat Res. 2019 Feb;477(2):322-323. doi: 10.1097/CORR.0000000000000415. Clin Orthop Relat Res. 2019. PMID: 30113337 Free PMC article. No abstract available.
Similar articles
-
Do 3-dimensional Spinopelvic Characteristics Normalize After THA? A Prospective, Comparative Study Using Motion Capture Analysis.Clin Orthop Relat Res. 2024 Sep 1;482(9):1642-1655. doi: 10.1097/CORR.0000000000003106. Epub 2024 May 14. Clin Orthop Relat Res. 2024. PMID: 39226524
-
Spinal Fusion Is Associated With Changes in Acetabular Orientation and Reductions in Pelvic Mobility.Clin Orthop Relat Res. 2019 Feb;477(2):324-330. doi: 10.1097/CORR.0000000000000390. Clin Orthop Relat Res. 2019. PMID: 30794220 Free PMC article.
-
Can spinopelvic mobility be predicted in patients awaiting total hip arthroplasty? A prospective, diagnostic study of patients with end-stage hip osteoarthritis.Bone Joint J. 2019 Aug;101-B(8):902-909. doi: 10.1302/0301-620X.101B8.BJJ-2019-0106.R1. Bone Joint J. 2019. PMID: 31362559 Clinical Trial.
-
Previous lumbar spine fusion increases the risk of dislocation following total hip arthroplasty in patients with hip-spine syndrome: a systematic review and meta-analysis.BMC Musculoskelet Disord. 2024 Sep 13;25(1):732. doi: 10.1186/s12891-024-07823-1. BMC Musculoskelet Disord. 2024. PMID: 39272046 Free PMC article.
-
Spinopelvic Compensatory Mechanisms for Reduced Hip Motion (ROM) in the Setting of Hip Osteoarthritis.Spine Deform. 2019 Nov;7(6):923-928. doi: 10.1016/j.jspd.2019.03.007. Spine Deform. 2019. PMID: 31732003 Review.
Cited by
-
Patient-Specific Acetabular Safe Zones in Total Hip Arthroplasty: External Validation of a Quantitative Approach to Preoperatively Templating Spinopelvic Parameters.Arthroplast Today. 2024 Oct 16;30:101508. doi: 10.1016/j.artd.2024.101508. eCollection 2024 Dec. Arthroplast Today. 2024. PMID: 39492998 Free PMC article.
-
CORR Insights®: 2018 Frank Stinchfield Award: Spinopelvic Hypermobility Is Associated With an Inferior Outcome After THA: Examining the Effect of Spinal Arthrodesis.Clin Orthop Relat Res. 2019 Feb;477(2):322-323. doi: 10.1097/CORR.0000000000000415. Clin Orthop Relat Res. 2019. PMID: 30113337 Free PMC article. No abstract available.
-
Lumbar spinal fusion does not increase early dislocation risk in primary total hip arthroplasty through the direct anterior approach.Arch Orthop Trauma Surg. 2022 Nov;142(11):3469-3475. doi: 10.1007/s00402-021-04203-5. Epub 2021 Oct 13. Arch Orthop Trauma Surg. 2022. PMID: 34643783
-
The Top Three Burning Questions in Total Hip Arthroplasty.Medicina (Kaunas). 2023 Mar 26;59(4):655. doi: 10.3390/medicina59040655. Medicina (Kaunas). 2023. PMID: 37109613 Free PMC article. Review.
-
Spinopelvic parameters in the lateral decubitus are different from standing and sitting positions.Sci Rep. 2025 Apr 26;15(1):14685. doi: 10.1038/s41598-025-98819-x. Sci Rep. 2025. PMID: 40287527 Free PMC article.
References
-
- Babisch JW, Layher F, Amiot LP. The rationale for tilt-adjusted acetabular cup navigation. J Bone Joint Surg Am. 2008;90:357–365. - PubMed
-
- Barry JJ, Sing DC, Vail TP, Hansen EN. Early outcomes of primary total hip arthroplasty after prior lumbar spinal fusion. J Arthroplasty. 2017;32:470–474. - PubMed
-
- Bedard NA, Martin CT, Slaven SE, Pugely AJ, Mendoza-Lattes SA, Callaghan JJ. Abnormally high dislocation rates of total hip arthroplasty after spinal deformity surgery. J Arthroplasty. 2016;31:2884–2885. - PubMed
-
- Bellamy N. Validation study of WOMAC: a health status instrument for measuring clinically-important patient-relevant outcomes following total hip or knee arthroplasty in osteoarthritis. J Orthop Rheumatol. 1988;1:95–108. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
