

Effectiveness of a multifactorial intervention for dizziness in older people in primary care: A cluster randomised controlled trial
- PMID: 30300371
- PMCID: PMC6178383
- DOI: 10.1371/journal.pone.0204876
Effectiveness of a multifactorial intervention for dizziness in older people in primary care: A cluster randomised controlled trial
Abstract
Objectives: Dizziness is common in older people. Physicians are often unable to identify a specific cause for dizziness in older people, even after an extensive diagnostic work-up. A prognosis-oriented approach, i.e. treating modifiable risk factors for an unfavourable course of dizziness, may reduce dizziness-related impairment in older people in primary care.
Design: Cluster randomized controlled trial.
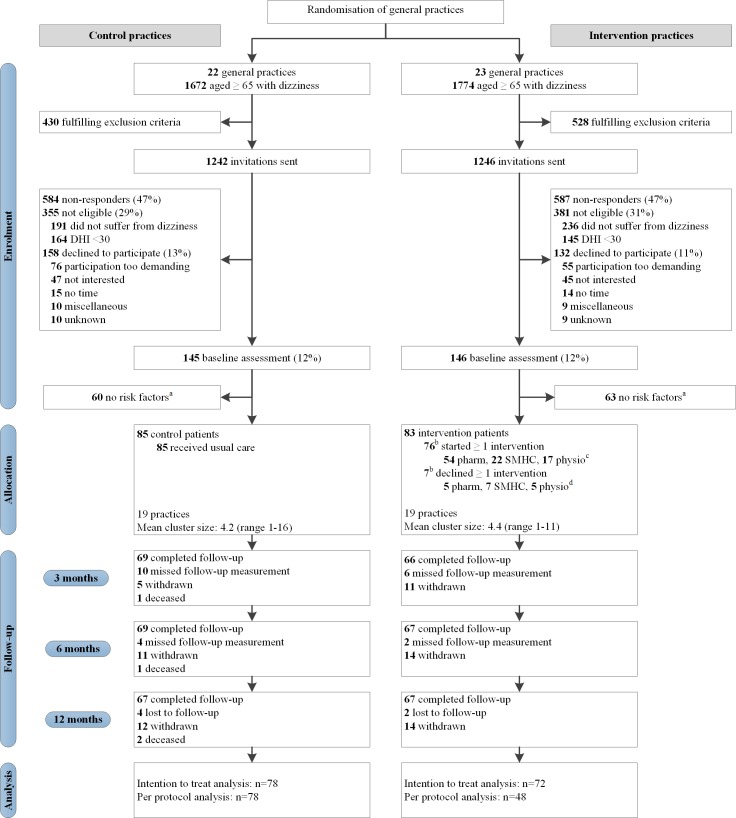
Setting: 45 primary care practices in The Netherlands.
Participants: 168 participants aged ≥65y who consulted their general practitioner for dizziness and experienced significant dizziness-related impairment (Dizziness Handicap Inventory (DHI) ≥30). Participants were part of to the intervention group (n = 83) or control group (n = 85), depending on whether they were enlisted in an intervention practice or in a control practice.
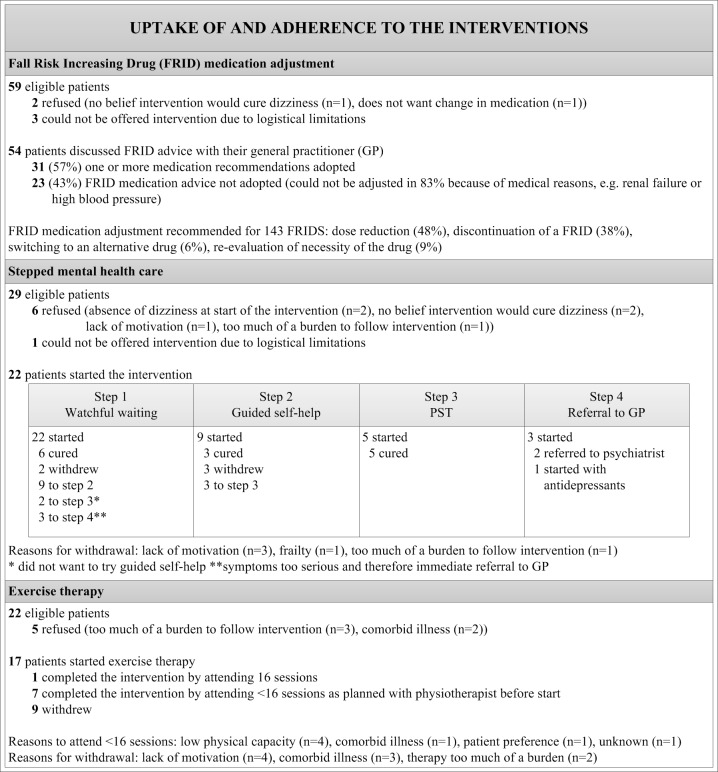
Interventions: The multifactorial intervention consisted of: medication adjustment in case of ≥3 prescribed fall-risk-increasing drugs (FRIDs) and/or stepped mental health care in case of anxiety disorder and/or depression and/or exercise therapy in case of impaired functional mobility. The intervention was compared to usual care.
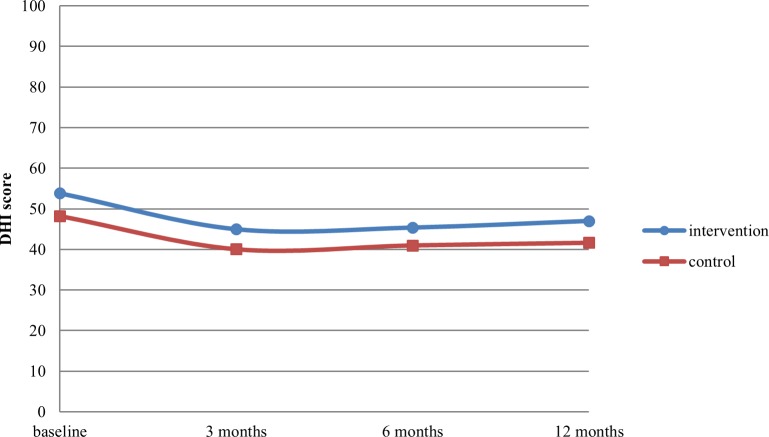
Outcome measures: The primary outcome was dizziness-related impairment. Secondary outcomes were quality of life (QoL), dizziness frequency, fall frequency, anxiety and depression, use of FRIDs.
Results: Intention-to-treat analysis showed no significant intervention effect on dizziness-related impairment (DHI score difference -0.69 [95% CI -5.66;4.28]; p = 0.79). The intervention proved effective in reducing the number of FRIDs (FRID difference -0.48 [95% CI -0.89;-0.06]; p = 0.02). No significant intervention effects were found on other secondary outcomes. The uptake of and adherence to the interventions was significantly lower in patients eligible for ≥2 interventions compared to patients eligible for one intervention (p<0.001).
Conclusions: The multifactorial intervention for dizziness in older patients showed no significant intervention effect on most outcomes and adherence to the multifactorial intervention was low. Although multifactorial treatment for older dizzy people seems promising in theory, we question its feasibility in daily practice. Future research could focus on a sequential treatment for dizziness, e.g. measuring effectiveness of various evidence-based therapies in a stepwise approach.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Aggarwal NT, Bennett DA, Bienias JL, Mendes de Leon CF, Morris MC, Evans DA. The prevalence of dizziness and its association with functional disability in a biracial community population. J Gerontol A Biol Sci Med Sci. 2000;55(5):M288–92. - PubMed
-
- Cigolle CT, Langa KM, Kabeto MU, Tian Z, Blaum CS. Geriatric conditions and disability: The Health and Retirement Study. Ann Intern Med. 2007;147(3):156–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
