

A Natural History of Actinic Keratosis and Cutaneous Squamous Cell Carcinoma Microbiomes
- PMID: 30301852
- PMCID: PMC6178618
- DOI: 10.1128/mBio.01432-18
A Natural History of Actinic Keratosis and Cutaneous Squamous Cell Carcinoma Microbiomes
Abstract
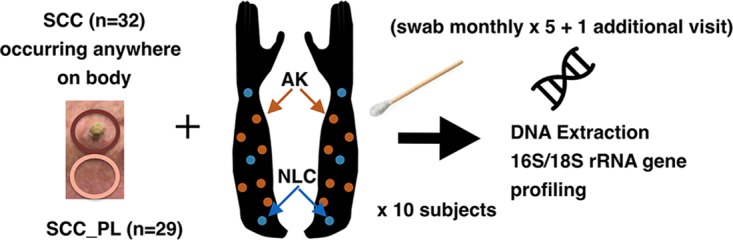
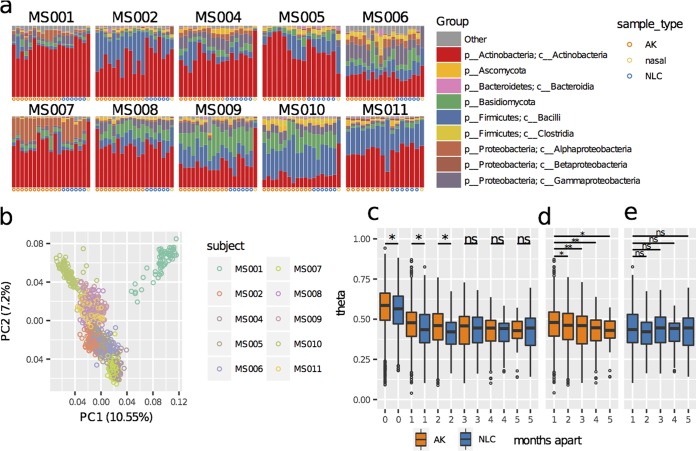
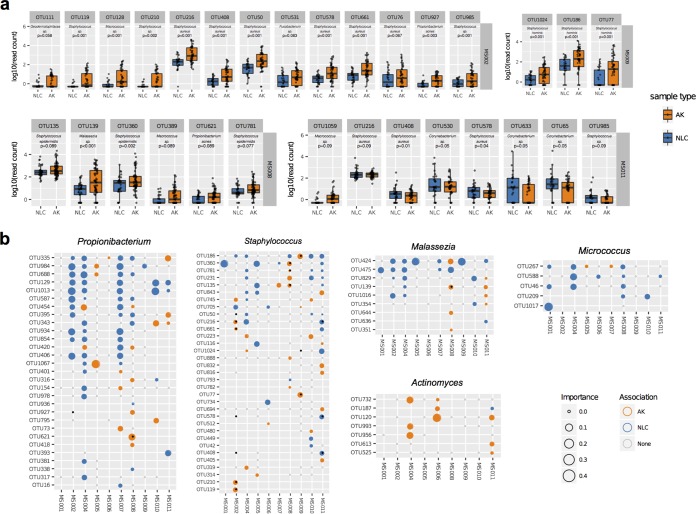
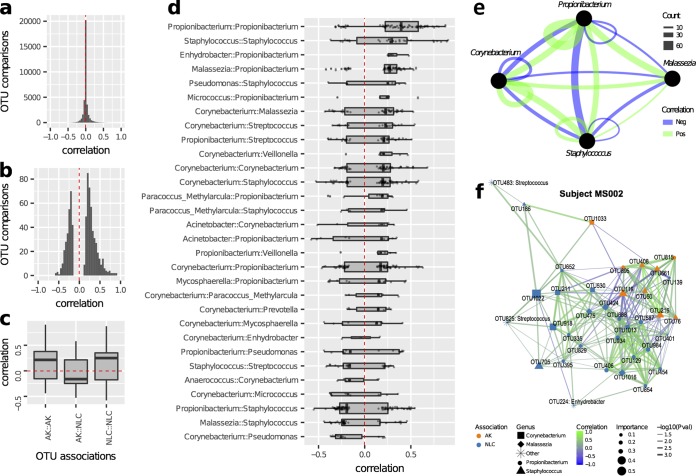
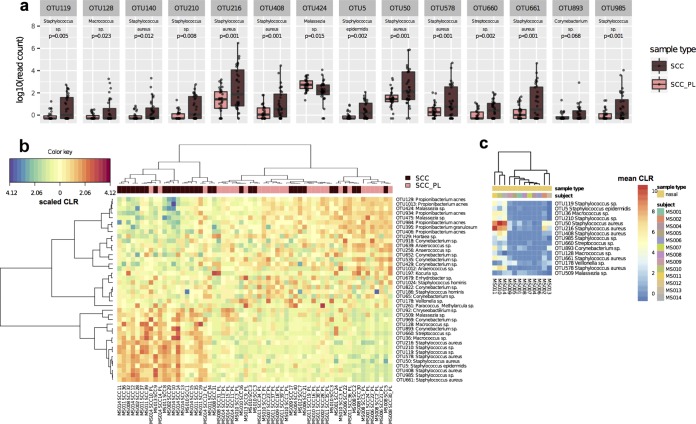
Cutaneous squamous cell carcinoma (SCC) is the second-most-common cancer in Australia. The majority of SCCs progress from premalignant actinic keratosis (AK) lesions that form on chronically sun-exposed skin. The role of skin microbiota in this progression is not well understood; therefore, we performed a longitudinal microbiome analysis of AKs and SCCs using a cohort of 13 SCC-prone immunocompetent men. The majority of variability in microbial profiles was attributable to subject, followed by time and lesion type. Propionibacterium and Malassezia organisms were relatively more abundant in nonlesional photodamaged skin than in AKs and SCCs. Staphylococcus was most commonly associated with lesional skin, in particular, sequences most closely related to Staphylococcus aureus Of 11 S. aureus-like operational taxonomic units (OTUs), six were significantly associated with SCC lesions across seven subjects, suggesting their specific involvement with AK-to-SCC progression. If a causative link exists between certain S. aureus-like OTUs and SCC etiology, therapeutic approaches specifically targeting these bacteria could be used to reduce SCC.IMPORTANCE Actinic keratosis (AK) and cutaneous squamous cell carcinoma (SCC) are two of the most common dermatologic conditions in Western countries and cause substantial morbidity worldwide. The role of human papillomaviruses under these conditions has been well studied yet remains inconclusive. One PCR-based study has investigated bacteria in the etiology of these conditions; however, no study has investigated the microbiomes of AK and SCC more broadly. We longitudinally profiled the microbiomes of 112 AK lesions, profiled cross sections of 32 spontaneously arising SCC lesions, and compared these to matching nonlesional photodamaged control skin sites. We identified commonly occurring strains of Propionibacterium and Malassezia at higher relative abundances on nonlesional skin than in AK and SCC lesions, and strains of Staphylococcus aureus were relatively more abundant in lesional than nonlesional skin. These findings may aid in the prevention of SCC.
Keywords: 16S RNA; Malassezia; Staphylococcus aureus; actinic keratosis; microbiome; skin; squamous cell carcinoma.
Copyright © 2018 Wood et al.
Figures
Similar articles
-
Characterization of the skin microbiome in normal and cutaneous squamous cell carcinoma affected cats and dogs.mSphere. 2024 Apr 23;9(4):e0055523. doi: 10.1128/msphere.00555-23. Epub 2024 Mar 26. mSphere. 2024. PMID: 38530017 Free PMC article.
-
Reduced Staphylococcus Abundance Characterizes the Lesional Microbiome of Actinic Keratosis Patients after Field-Directed Therapies.Microbiol Spectr. 2023 Jun 15;11(3):e0440122. doi: 10.1128/spectrum.04401-22. Epub 2023 May 22. Microbiol Spectr. 2023. PMID: 37212689 Free PMC article.
-
Gene expression patterns of normal human skin, actinic keratosis, and squamous cell carcinoma: a spectrum of disease progression.Arch Dermatol. 2010 Mar;146(3):288-93. doi: 10.1001/archdermatol.2009.378. Arch Dermatol. 2010. PMID: 20231500
-
Progression of actinic keratosis to squamous cell carcinoma revisited: clinical and treatment implications.Cutis. 2011 Apr;87(4):201-7. Cutis. 2011. PMID: 21644496 Review.
-
Management of actinic keratosis at specific body sites in patients at high risk of carcinoma lesions: expert consensus from the AKTeam™ of expert clinicians.J Eur Acad Dermatol Venereol. 2018 Mar;32(3):339-346. doi: 10.1111/jdv.14753. Epub 2018 Jan 15. J Eur Acad Dermatol Venereol. 2018. PMID: 29235161
Cited by
-
Secreted Toxins From Staphylococcus aureus Strains Isolated From Keratinocyte Skin Cancers Mediate Pro-tumorigenic Inflammatory Responses in the Skin.Front Microbiol. 2022 Jan 25;12:789042. doi: 10.3389/fmicb.2021.789042. eCollection 2021. Front Microbiol. 2022. PMID: 35145494 Free PMC article.
-
Role of Nicotinamide in the Pathogenesis of Actinic Keratosis: Implications for NAD+/SIRT1 Pathway.Biomolecules. 2024 Nov 27;14(12):1512. doi: 10.3390/biom14121512. Biomolecules. 2024. PMID: 39766219 Free PMC article.
-
Challenges in exploring and manipulating the human skin microbiome.Microbiome. 2021 May 30;9(1):125. doi: 10.1186/s40168-021-01062-5. Microbiome. 2021. PMID: 34053468 Free PMC article. Review.
-
From Dysbiosis to Healthy Skin: Major Contributions of Cutibacterium acnes to Skin Homeostasis.Microorganisms. 2021 Mar 18;9(3):628. doi: 10.3390/microorganisms9030628. Microorganisms. 2021. PMID: 33803499 Free PMC article. Review.
-
Topical Treatment of Actinic Keratosis and Metalloproteinase Expression: A Clinico-Pathological Retrospective Study.Int J Mol Sci. 2022 Sep 26;23(19):11351. doi: 10.3390/ijms231911351. Int J Mol Sci. 2022. PMID: 36232651 Free PMC article.
References
-
- Bouwes Bavinck JN, Euvrard S, Naldi L, Nindl I, Proby CM, Neale R, Abeni D, Tessari GP, Feltkamp MCW, Claudy A, Stockfleth E, Harwood CA. 2007. Keratotic skin lesions and other risk factors are associated with skin cancer in organ-transplant recipients: a case-control study in The Netherlands, United Kingdom, Germany, France, and Italy. J Invest Dermatol 127:1647–1656. doi:10.1038/sj.jid.5700776. - DOI - PMC - PubMed
-
- Landis ET, Davis SA, Taheri A, Feldman SR. 2014. Top dermatologic diagnoses by age. Dermatol Online J 20:22368. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
