

Persistent platelet activation and apoptosis in virologically suppressed HIV-infected individuals
- PMID: 30301959
- PMCID: PMC6178345
- DOI: 10.1038/s41598-018-33403-0
Persistent platelet activation and apoptosis in virologically suppressed HIV-infected individuals
Abstract
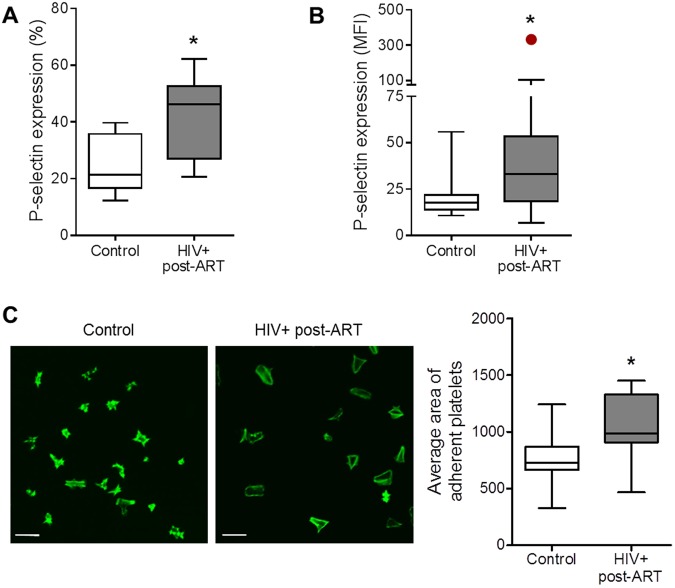
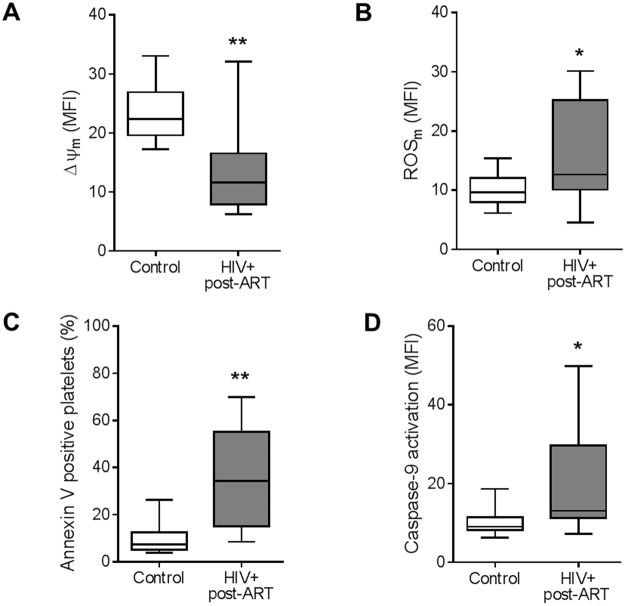
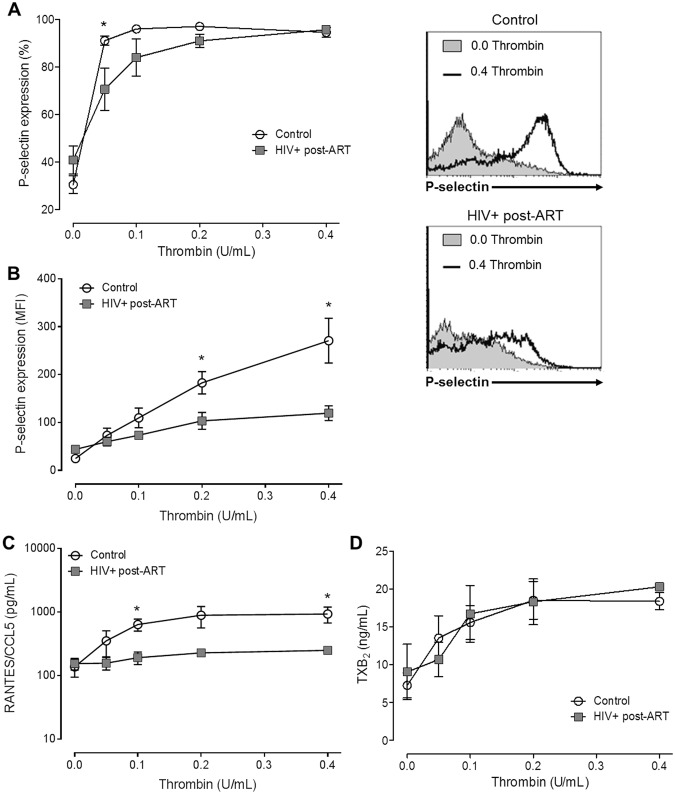
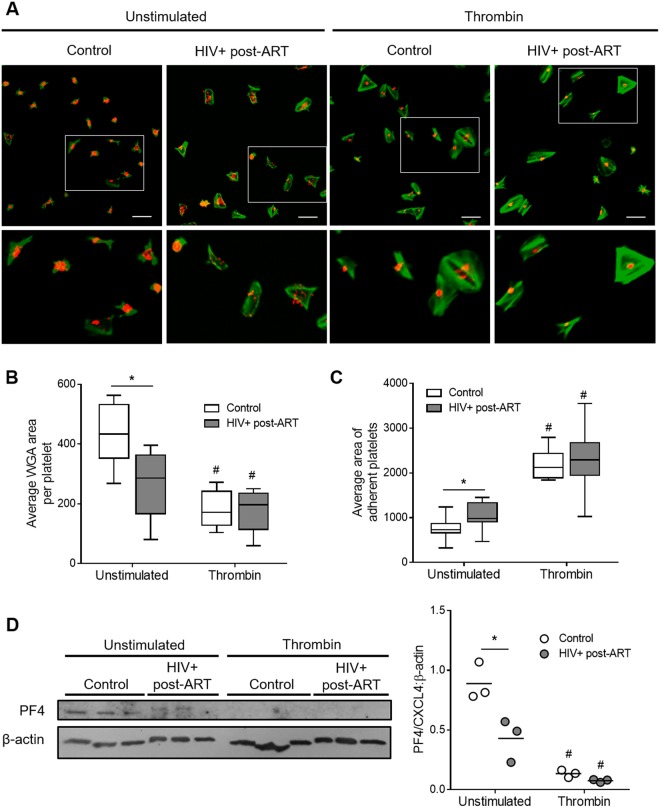
Cardiovascular diseases and thrombotic events became major clinical problems in the combined antiretroviral therapy (cART) era. Although the precise mechanisms behind these clinical problems have not been fully elucidated, a persistent pro-inflammatory state plays a central role. As platelets play important roles on both, thrombus formation and inflammatory/immune response, we aimed at investigating platelet function in HIV-infected subjects virologically controlled through cART. We evaluate parameters of activation, mitochondrial function and activation of apoptosis pathways in platelets from 30 HIV-infected individuals under stable cART and 36 healthy volunteers. Despite viral control achieved through cART, HIV-infected individuals exhibited increased platelet activation as indicated by P-selectin expression and platelet spreading when adhered on fibrinogen-coated surfaces. Platelets from HIV-infected subjects also exhibited mitochondrial dysfunction and activation of apoptosis pathways. Finally, thrombin stimuli induced lower levels of P-selectin translocation and RANTES secretion, but not TXA2 synthesis, in platelets from HIV-infected individuals compared to control; and labeling of platelet alpha granules showed reduced granule content in platelets from HIV-infected individuals when compared to healthy subjects. In summary, platelets derived from HIV-infected individuals under stable cART exhibit a phenotype of increased activation, activation of the intrinsic pathway of apoptosis and undermined granule secretion in response to thrombin.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Lewden C, et al. HIV-infected adults with a CD4 cell count greater than 500 cells/mm3 on long-term combination antiretroviral therapy reach same mortality rates as the general population. J Acquir Immune Defic Syndr. 2007;46(1):72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
