

Spinal epidural lipomatosis presenting to a U.S. Veterans Affairs pain and rehabilitation department: a report of two cases
- PMID: 30302238
- PMCID: PMC6167793
- DOI: 10.1186/s12998-018-0203-1
Spinal epidural lipomatosis presenting to a U.S. Veterans Affairs pain and rehabilitation department: a report of two cases
Abstract
Background: Spinal epidural lipomatosis is an uncommon source of neurogenic claudication. We present two cases of spinal epidural lipomatosis as it relates to diagnosis, management, and a possible association with common medical intervention.
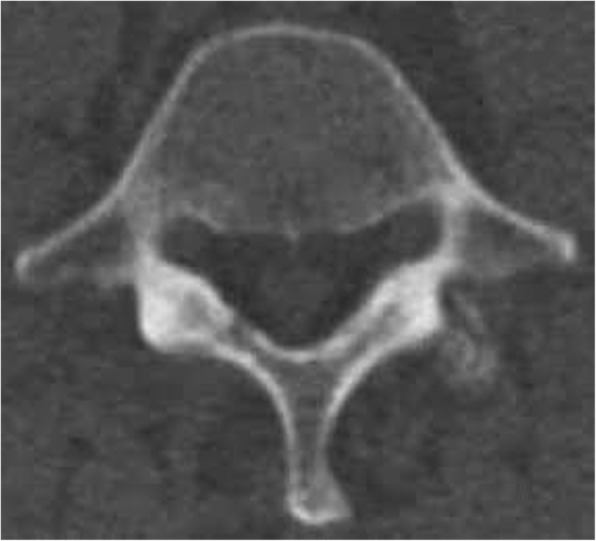
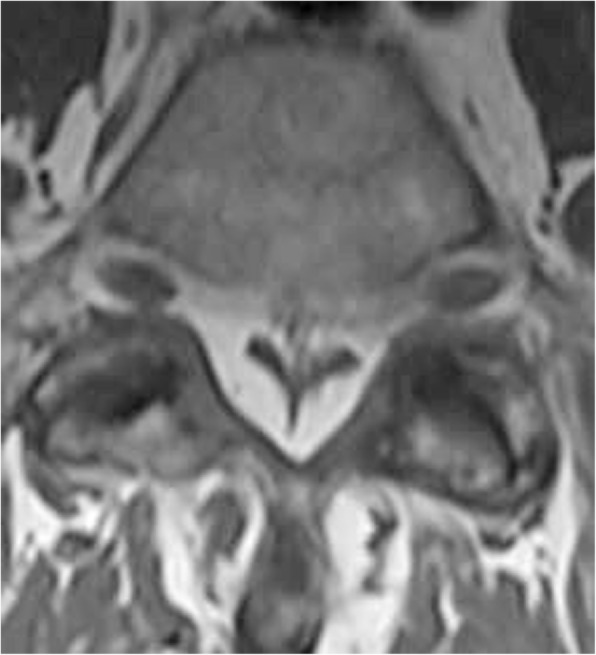
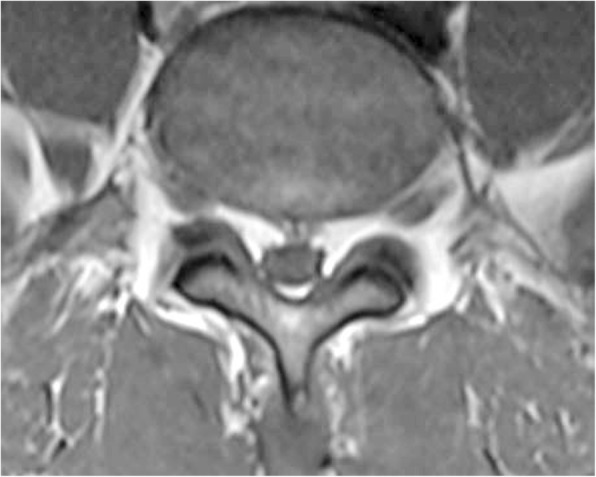
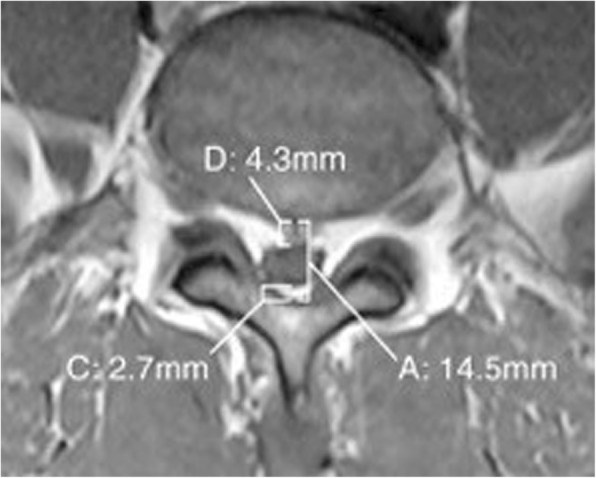
Case presentation: Case 1: 63-year old male patient presented with neurogenic claudication symptoms, but without evidence of bony central canal stenosis on lumbar computed tomography. He entered a trial of spinal manipulation with transient beneficial gains after seven appointments, but no durable change in neurogenic claudication. An MRI was recommended at this point which revealed grade III spinal epidural lipomatosis at the L5/S1 level.Case 2: 51-year old male patient presented to a pain management physician with radicular symptoms for a series of lumbar epidural steroid injections. He completed a series of three lumbar epidural steroid injections with only short-term benefit. A repeat MRI demonstrated the presence of grade I (borderline grade II) spinal epidural lipomatosis.
Conclusions: The first case illustrates a limitation of ruling out central canal stenosis with computed tomography for patients unable to undergo an MRI. The second case demonstrates a possible association between steroid injections and spinal epidural lipomatosis. An association of this kind has not been established; further research is needed to determine the significance.
Keywords: Case series; Chiropractic; Epidural fat; Epidural steroid injection; Lipomatosis; Spinal stenosis.
Conflict of interest statement
KMS performed literature review and prepared the manuscript. CJD provided patient care and assisted in preparation of the manuscript. GAB and PJW provided supervision and editorial review. JDT provided patient care and editorial review. All authors’ read and approved the final manuscript.The Saint Louis Veterans Health Affairs privacy officer and Research Development Committee provided approval for publication of this report and associated images.Written informed consent was obtained from the patients for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.The authors declare they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- Koch CA, Doppman JL, Patronas NJ, Nieman LK, Chrousis GP. Do glucocorticoids cause spinal epidural lipomatosis? When endocrinology and spinal surgery meet. TEM. 2000;11(3):86–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
