

Successful treatment of steroid-refractory double-positive ANCA and anti-GBM disease with a combination of plasma exchange and immunosuppression: A case report and literature review
- PMID: 30302307
- PMCID: PMC6174835
- DOI: 10.1016/j.rmcr.2018.09.016
Successful treatment of steroid-refractory double-positive ANCA and anti-GBM disease with a combination of plasma exchange and immunosuppression: A case report and literature review
Abstract
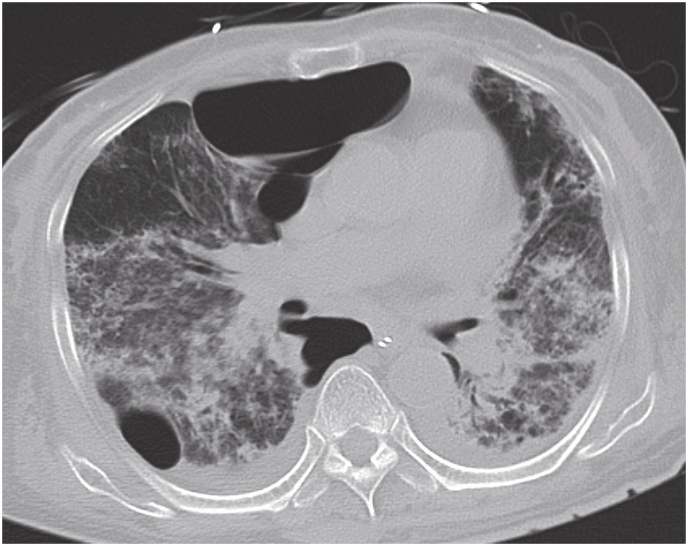
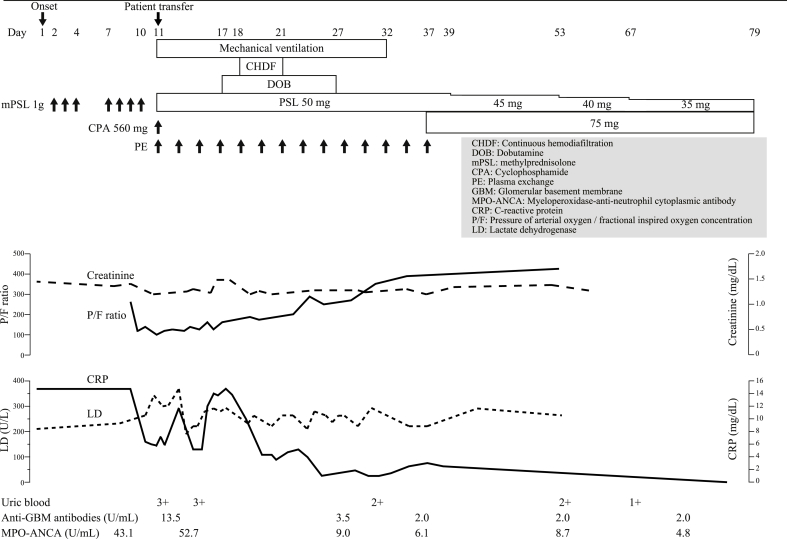
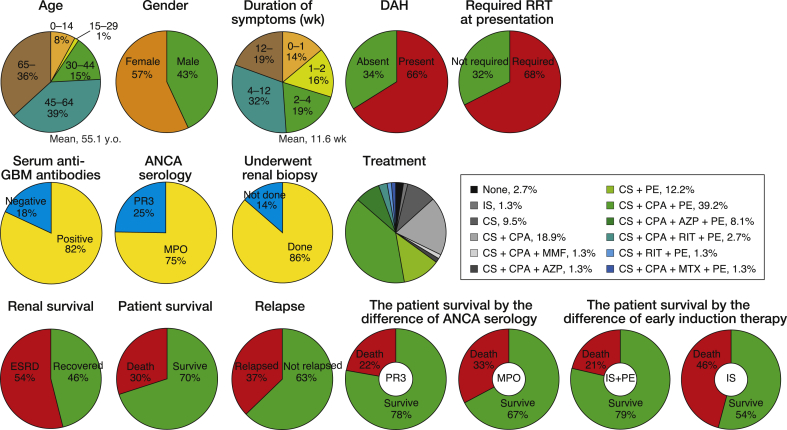
The concurrence of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) and anti-glomerular basement membrane (GBM) disease, known as double-positive disease, is rare, but it occurs at a much higher frequency than expected by chance. Double-positive disease has an aggressive clinical course, with no optimal treatment strategy. Here we describe a patient with steroid-refractory double-positive disease who was treated successfully with the addition of plasma exchange (PE) and cyclophosphamide (CPA). A 78-year-old Japanese woman who was diagnosed with diffuse alveolar hemorrhage and rapidly progressive glomerulonephritis received two cycles of pulse steroid therapy. However, her respiratory and renal condition deteriorated. She was found to be positive for both myeloperoxidase-ANCA and anti-GBM antibodies. The combination of PE and CPA improved her systemic condition. This is the first case report of a patient with steroid-refractory double-positive disease who was successfully treated with the addition of PE and CPA. The marked contrast in therapeutic response to corticosteroids alone and the addition of PE and CPA in this case strongly implies that earlier induction of combination therapy aimed at rapid removal of pathogenic autoantibodies and prevention of ongoing antibody production might improve the outcome of this life-threatening disease.
Keywords: Anti-glomerular basement membrane disease; Antineutrophil cytoplasmic antibody-associated vasculitis; Double-positive disease; Immunosuppression; Plasma exchange; Relapse.
Figures
Similar articles
-
Sequential occurrence of microscopic polyangiitis and anti-glomerular basement membrane disease in a patient with small cell lung cancer: a case report.J Med Case Rep. 2021 Feb 1;15(1):30. doi: 10.1186/s13256-020-02614-3. J Med Case Rep. 2021. PMID: 33517889 Free PMC article.
-
MPO-ANCA-positive anti-glomerular basement membrane antibody disease successfully treated by plasma exchange and immunosuppressive therapy.Ren Fail. 2011;33(6):626-31. doi: 10.3109/0886022X.2011.581401. Epub 2011 May 20. Ren Fail. 2011. PMID: 21599422
-
A relapsing case of pulmonary-renal syndrome after a sequential rise in MPO-ANCA and anti-GBM antibodies.CEN Case Rep. 2019 Aug;8(3):221-225. doi: 10.1007/s13730-019-00397-1. Epub 2019 Apr 3. CEN Case Rep. 2019. PMID: 30945174 Free PMC article.
-
Goodpasture's disease: a report of ten cases and a review of the literature.Autoimmun Rev. 2013 Sep;12(11):1101-8. doi: 10.1016/j.autrev.2013.06.014. Epub 2013 Jun 24. Autoimmun Rev. 2013. PMID: 23806563 Review.
-
Antiglomerular Basement Membrane Disease.Semin Respir Crit Care Med. 2018 Aug;39(4):494-503. doi: 10.1055/s-0038-1669413. Epub 2018 Nov 7. Semin Respir Crit Care Med. 2018. PMID: 30404116 Review.
Cited by
-
Management of Double-Seropositive Anti-Glomerular Basement Membrane and Anti-Neutrophil Cytoplasmic Antibodies with 100% Crescentic Glomerulonephritis and Nephrotic Range Proteinuria in a Young Female.Biomedicines. 2024 Apr 19;12(4):906. doi: 10.3390/biomedicines12040906. Biomedicines. 2024. PMID: 38672260 Free PMC article.
-
Therapeutics controversies in antineutrophilic cytoplasmic antibody-associated vasculitis.Clin Exp Nephrol. 2025 May 20. doi: 10.1007/s10157-025-02693-w. Online ahead of print. Clin Exp Nephrol. 2025. PMID: 40392453 Review.
-
Clinical features and prognosis of MPO-ANCA and anti-GBM double-seropositive patients.Front Immunol. 2022 Oct 27;13:991469. doi: 10.3389/fimmu.2022.991469. eCollection 2022. Front Immunol. 2022. PMID: 36389826 Free PMC article.
-
Sequential occurrence of microscopic polyangiitis and anti-glomerular basement membrane disease in a patient with small cell lung cancer: a case report.J Med Case Rep. 2021 Feb 1;15(1):30. doi: 10.1186/s13256-020-02614-3. J Med Case Rep. 2021. PMID: 33517889 Free PMC article.
-
A Rare Case of Double Antibody-Positive Rapidly Progressive Glomerulonephritis: A Therapeutic Challenge.J Investig Med High Impact Case Rep. 2021 Jan-Dec;9:23247096211013193. doi: 10.1177/23247096211013193. J Investig Med High Impact Case Rep. 2021. PMID: 33966476 Free PMC article.
References
-
- Bosch X., Guilabert A., Espinosa G., Mirapeix E. Treatment of antineutrophil cytoplasmic antibody associated vasculitis: a systematic review. J. Am. Med. Assoc. 2007;298:655–669. - PubMed
-
- Jennette J.C., Falk R.J., Bacon P.A., Basu N., Cid M.C., Ferrario F., Flores-Suarez L.F., Gross W.L., Guillevin L., Hagen E.C., Hoffman G.S., Jayne D.R., Kallenberg C.G., Lamprecht P., Langford C.A., Luqmani R.A., Mahr A.D., Matteson E.L., Merkel P.A., Ozen S., Pusey C.D., Rasmussen N., Rees A.J., Scott D.G., Specks U., Stone J.H., Takahashi K., Watts R.A. 2012 revised international Chapel hill Consensus Conference nomenclature of vasculitides. Arthritis Rheum. 2013;65:1–11. - PubMed
-
- Jayne D.R., Marshall P.D., Jones S.J., Lockwood C.M. Autoantibodies to GBM and neutrophil cytoplasm in rapidly progressive glomerulonephritis. Kidney Int. 1990;37:965–970. - PubMed
-
- Levy J.B., Hammad T., Coulthart A., Dougan T., Pusey C.D. Clinical features and outcome of patients with both ANCA and anti-GBM antibodies. Kidney Int. 2004;66:1535–1540. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
