

Comparison of allogeneic and autogenous bone grafts for augmentation of alveolar ridge defects-A 12-month retrospective radiographic evaluation
- PMID: 30303581
- PMCID: PMC6282851
- DOI: 10.1111/clr.13380
Comparison of allogeneic and autogenous bone grafts for augmentation of alveolar ridge defects-A 12-month retrospective radiographic evaluation
Abstract
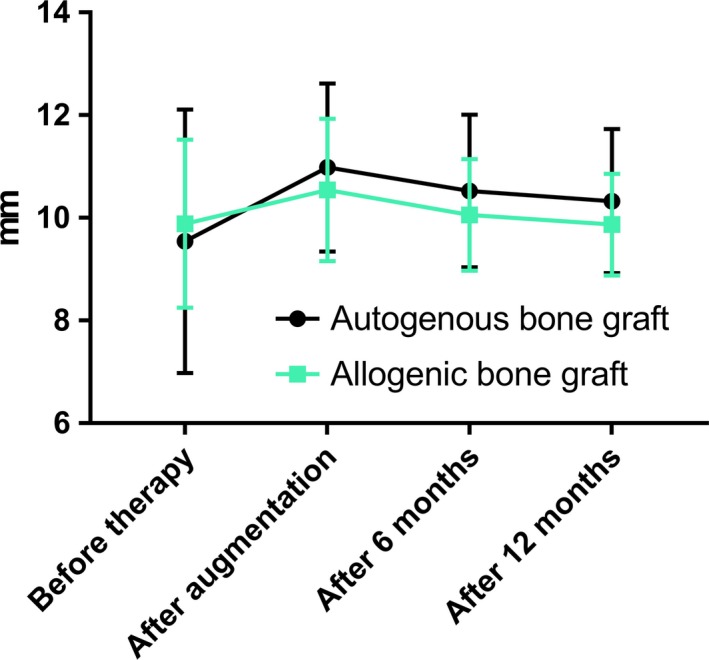
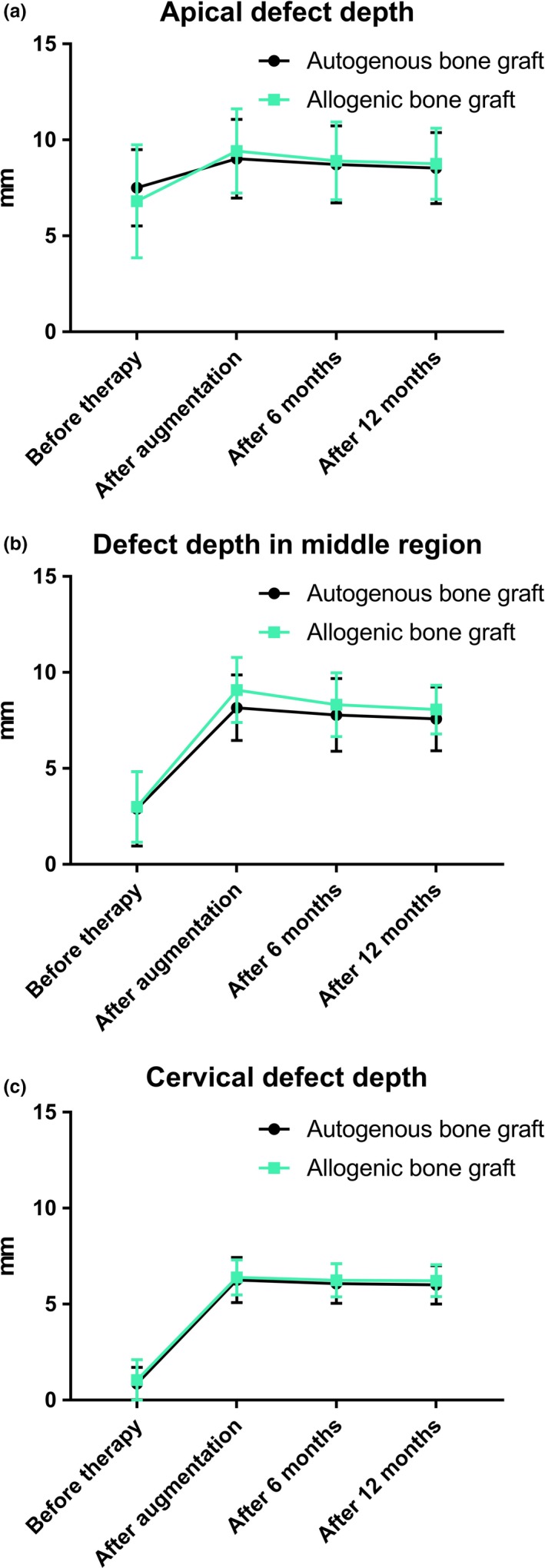
Objectives: The aim of this study was to compare three-dimensional alterations following the use of autogenous versus allogeneic onlay grafts for augmentation at single tooth defects.
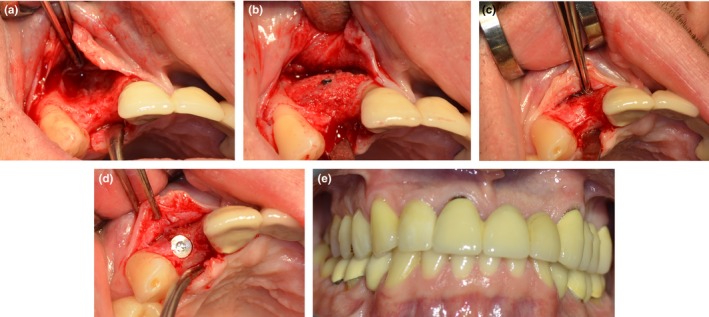
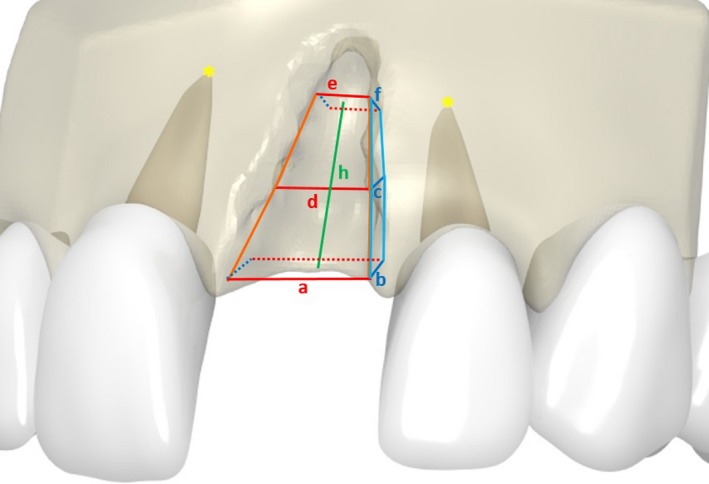
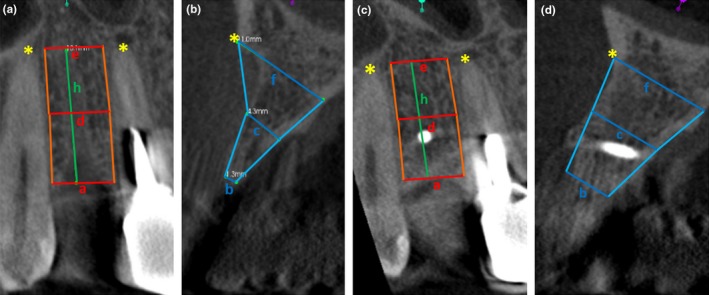
Materials and methods: Alveolar bone width at specific implant sites were assessed using sagittal and cross-sectional CBCT images prior grafting and at three subsequent time points. Twenty-one patients received autogenous bone blocks harvested from the retromolar region and another 21 patients received freeze-dried cancellous allogeneic bone blocks.
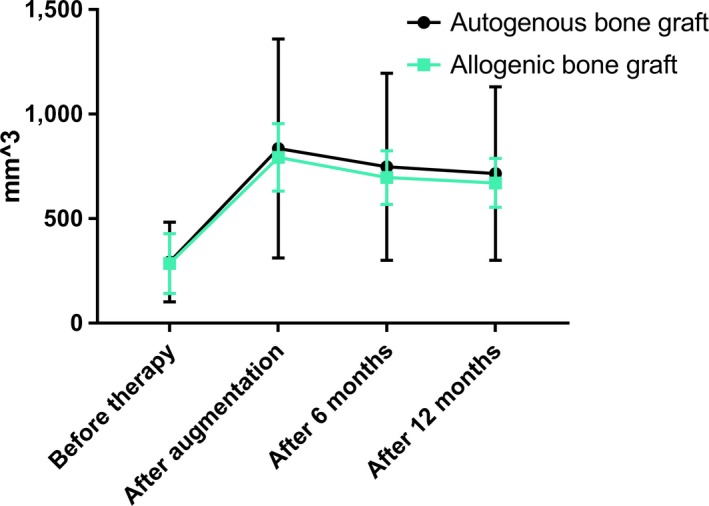
Results: The vertical and horizontal dimensions did not significantly differ between autogenous and allogeneic bone grafts at any time point. In addition, there were no statistically significant differences in graft remodeling rates between autogenous (mean shrinkage rate after 12 months: 12.5% ± 7.8%) and allogeneic onlay grafts (mean shrinkage rate after 12 months: 14.4% ± 9.8%).
Conclusions: Freeze-dried cancellous allogeneic bone blocks showed equivalent volumetric shrinkage rates as autogenous bone blocks when used for treating circumscribed bone defects classified as Type-II to Type-IV according to the ITI-treatment guide categories. Therefore, it is not necessary to over-contour the alveolar ridge when using allogeneic blocks for treating single tooth defects, but to apply the same procedure as when using autogenous blocks.
Keywords: allogeneic; alveolar ridge defect; augmentation; autogenous; dental implants; graft remodeling.
© 2018 The Authors. Clinical Oral Implants Research Published by John Wiley & Sons Ltd.
Figures


References
-
- Al‐Abedalla, K. , Torres, J. , Cortes, A. R. , Wu, X. , Nader, S. A. , Daniel, N. , & Tamimi, F. (2015). Bone augmented with allograft onlays for implant placement could be comparable with native bone. Journal of Oral and Maxillofacial Surgery, 73(11), 2108–2122. 10.1016/j.joms.2015.06.151 - DOI - PubMed
-
- Aslan, E. , Gultekin, A. , Karabuda, C. , Mortellaro, C. , Olgac, V. , & Mijiritsky, E. (2016). Clinical, histological, and histomorphometric evaluation of demineralized freeze‐dried cortical block allografts for alveolar ridge augmentation. Journal of Craniofacial Surgery, 27(5), 1181–1186. 10.1097/SCS.0000000000002548 - DOI - PubMed
-
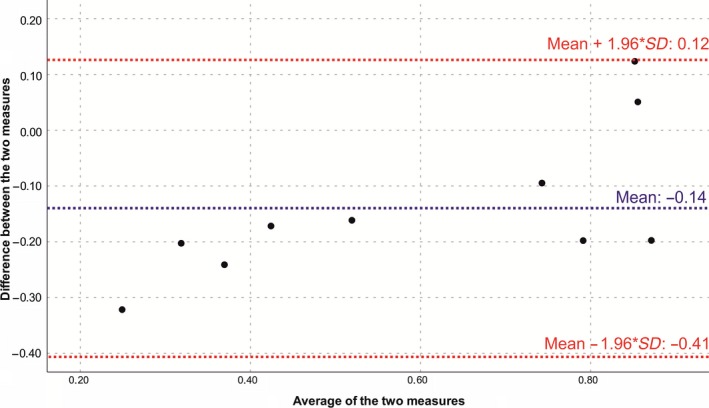
- Bland, J. M. , & Altman, D. G. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. Lancet, 1(8476), 307–310. S0140-6736(86)90837-8[pii] - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
