

Long-term Oncological and Functional Outcomes of Chemoradiotherapy Followed by Organ-Sparing Transanal Endoscopic Microsurgery for Distal Rectal Cancer: The CARTS Study
- PMID: 30304338
- PMCID: PMC6439861
- DOI: 10.1001/jamasurg.2018.3752
Long-term Oncological and Functional Outcomes of Chemoradiotherapy Followed by Organ-Sparing Transanal Endoscopic Microsurgery for Distal Rectal Cancer: The CARTS Study
Abstract
Importance: Treatment of rectal cancer is shifting toward organ preservation aiming to reduce surgery-related morbidity. Short-term outcomes of organ-preserving strategies are promising, but long-term outcomes are scarce in the literature.
Objective: To explore long-term oncological outcomes and health-related quality of life (HRQL) in patients with cT1-3N0M0 rectal cancer who underwent neoadjuvant chemoradiotherapy (CRT) followed by transanal endoscopic microsurgery (TEM).
Design, setting, and participants: In this multicenter phase II feasibility study, patients with cT1-3N0M0 rectal cancer admitted to referral centers for rectal cancer throughout the Netherlands between February 2011 and September 2012 were prospectively included. These patients were to be treated with neoadjuvant CRT followed by TEM in case of good response. An intensive follow-up scheme was used to detect local recurrences and/or distant metastases. Data from validated HRQL questionnaires and low anterior resection syndrome questionnaires were collected. Data were analyzed from February 2011 to April 2017.
Main outcomes and measures: The primary study outcome of the study was the number of ypT0-1 specimens by performing TEM. Secondary outcome parameters were locoregional recurrences and HRQL.
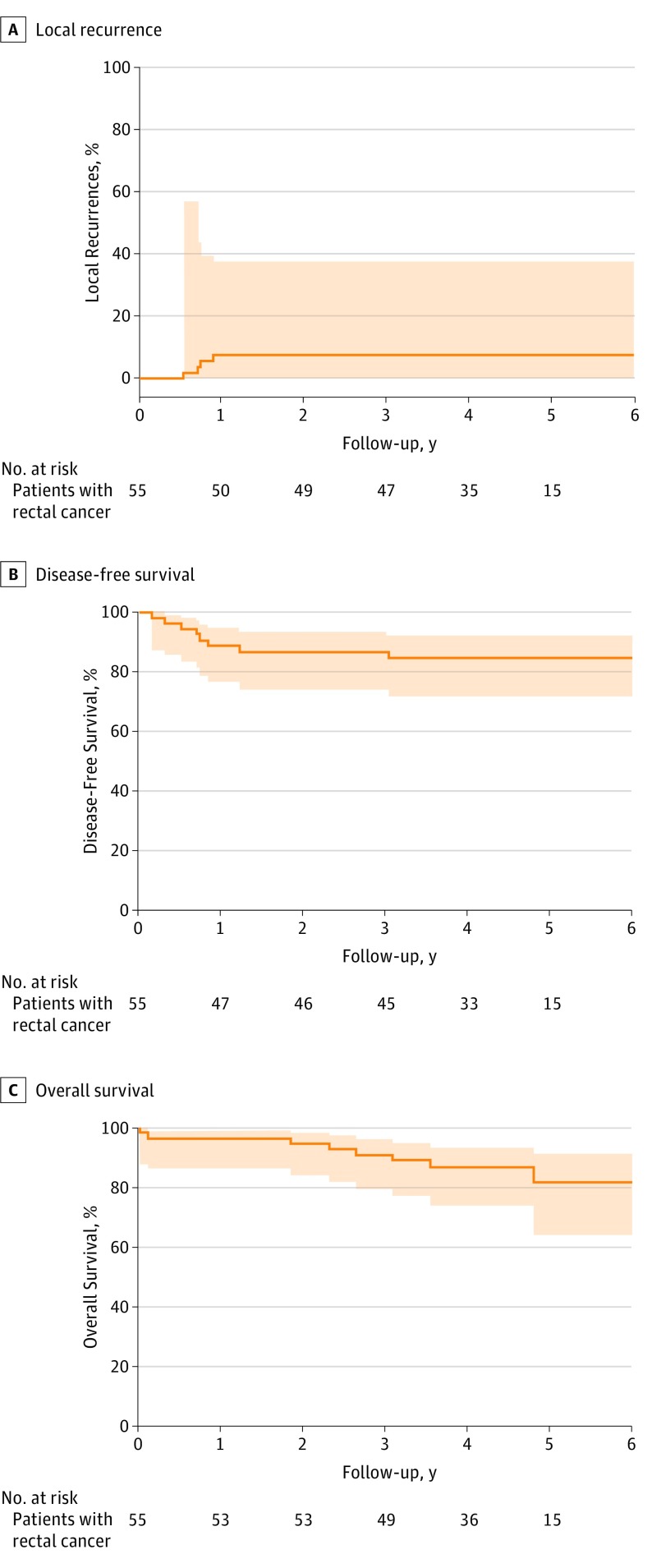
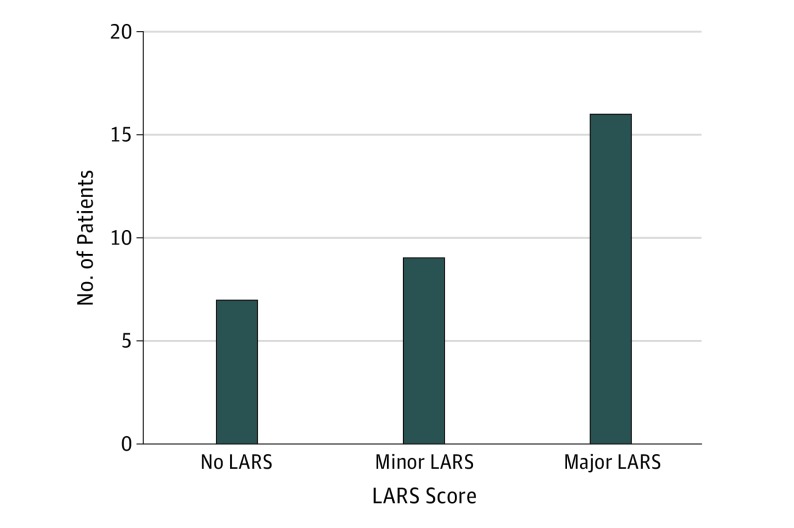
Results: Of the 55 included patients, 30 (55%) were male, and the mean (SD) age was 64 (39-82) years. Patients were followed up for a median (interquartile range) period of 53 (39-57) months. Two patients (4%) died during CRT, 1 (2%) stopped CRT, and 1 (2%) was lost to follow-up. Following CRT, 47 patients (85%) underwent TEM, of whom 35 (74%) were successfully treated with local excision alone. Total mesorectal excision was performed in 16 patients (4 with inadequate responses, 8 with completion after TEM, and 4 with salvage for local recurrence). The actuarial 5-year local recurrence rate was 7.7%, with 5-year disease-free and overall survival rates of 81.6% and 82.8%, respectively. Health-related quality of life during follow-up was equal to baseline, with improved emotional well-being in patients treated with local excision (mean score at baseline, 72.0; 95% CI, 67.1-80.1; mean score at follow-up, 86.9; 95% CI, 79.2-94.7; P = .001). Major, minor, and no low anterior resection syndrome was experienced in 50%, 28%, and 22%, respectively, of patients with successful organ preservation.
Conclusions and relevance: In early-stage rectal cancer (cT1-3N0M0), CRT enables organ preservation with additional TEM surgery in approximately two-thirds of patients with good long-term oncological outcome and HRQL. This multimodality treatment triggers a certain degree of bowel dysfunction, and one-third of patients still undergo radical surgery and are overtreated by CRT.
Conflict of interest statement
Figures
Comment in
-
Chemoradiotherapy and Local Excision for Organ Preservation in Early Rectal Cancer-The End of the Beginning?JAMA Surg. 2019 Jan 1;154(1):54-55. doi: 10.1001/jamasurg.2018.3760. JAMA Surg. 2019. PMID: 30304376 No abstract available.
-
Gastrointestinal Cancers: Fine-Tuning the Management of Rectal, Esophageal, and Pancreas Cancers.Int J Radiat Oncol Biol Phys. 2019 Sep 1;105(1):1-10. doi: 10.1016/j.ijrobp.2019.04.037. Int J Radiat Oncol Biol Phys. 2019. PMID: 31422802 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
