

Frequency and Associations of Prescription Nonsteroidal Anti-inflammatory Drug Use Among Patients With a Musculoskeletal Disorder and Hypertension, Heart Failure, or Chronic Kidney Disease
- PMID: 30304456
- PMCID: PMC6248204
- DOI: 10.1001/jamainternmed.2018.4273
Frequency and Associations of Prescription Nonsteroidal Anti-inflammatory Drug Use Among Patients With a Musculoskeletal Disorder and Hypertension, Heart Failure, or Chronic Kidney Disease
Abstract
Importance: International nephrology societies advise against nonsteroidal anti-inflammatory drug (NSAID) use in patients with hypertension, heart failure, or chronic kidney disease (CKD); however, recent studies have not investigated the frequency or associations of use in these patients.
Objectives: To estimate the frequency of and variation in prescription NSAID use among high-risk patients, to identify characteristics associated with prescription NSAID use, and to investigate whether use is associated with short-term, safety-related outcomes.
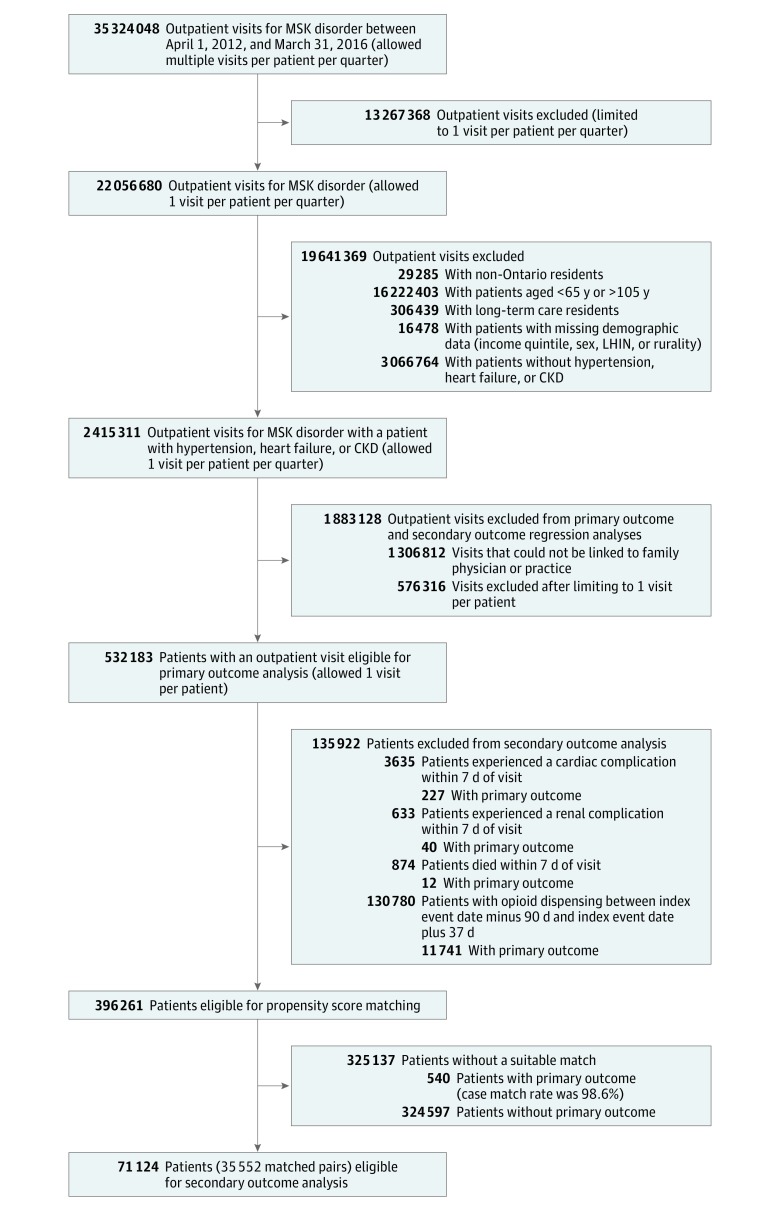
Design, setting, and participants: In this retrospective cohort study, administrative claims databases were linked to create a cohort of primary care visits for a musculoskeletal disorder involving patients 65 years and older with a history of hypertension, heart failure, or CKD between April 1, 2012, and March 31, 2016, in Ontario, Canada.
Exposure: Prescription NSAID use was defined as at least 1 patient-level Ontario Drug Benefit claim for a prescription NSAID dispensing within 7 days after a visit.
Main outcomes and measures: Multiple cardiovascular and renal safety-related outcomes were observed between 8 and 37 days after each visit, including cardiac complications (any emergency department visit or hospitalization for cardiovascular disease), renal complications (any hospitalization for hyperkalemia, acute kidney injury, or dialysis), and death.
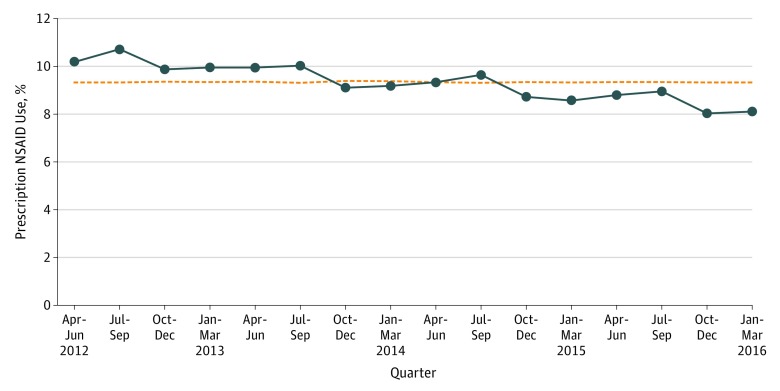
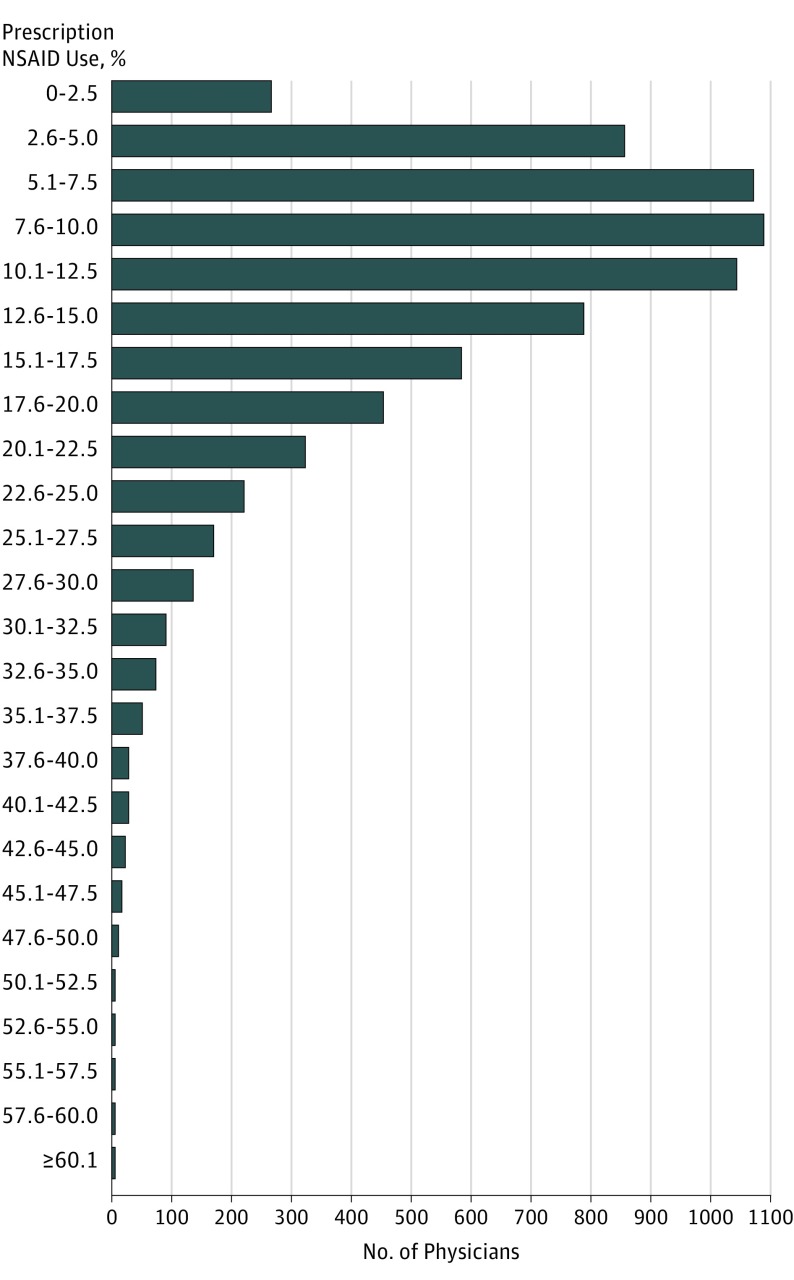
Results: The study identified 2 415 291 musculoskeletal-related primary care visits by 814 049 older adults (mean [SD] age, 75.3 [4.0] years; 61.1% female) with hypertension, heart failure, or CKD, of which 224 825 (9.3%) were followed by prescription NSAID use. The median physician-level prescribing rate was 11.0% (interquartile range, 6.7%-16.7%) among 7365 primary care physicians. Within a sample of 35 552 matched patient pairs, each consisting of an exposed and nonexposed patient matched on the logit of their propensity score for prescription NSAID use (exposure), the study found similar rates of cardiac complications (288 [0.8%] vs 279 [0.8%]), renal complications (34 [0.1%] vs 33 [0.1%]), and death (27 [0.1%] vs 30 [0.1%]). For cardiovascular and renal-safety related outcomes, there was no difference between exposed patients (308 [0.9%]) and nonexposed patients (300 [0.8%]) (absolute risk reduction, 0.0003; 95% CI, -0.001 to 0.002; P = .74).
Conclusions and relevance: While prescription NSAID use in primary care was frequent among high-risk patients, with widespread physician-level variation, use was not associated with increased risk of short-term, safety-related outcomes.
Conflict of interest statement
Figures
Comment in
-
Studying Drug Safety in the Real World.JAMA Intern Med. 2018 Nov 1;178(11):1533-1534. doi: 10.1001/jamainternmed.2018.5766. JAMA Intern Med. 2018. PMID: 30304435 No abstract available.
-
Association of NSAID Use and Renal Complications.JAMA Intern Med. 2019 Apr 1;179(4):586. doi: 10.1001/jamainternmed.2018.8684. JAMA Intern Med. 2019. PMID: 30933223 No abstract available.
-
Association of NSAID Use and Renal Complications-Reply.JAMA Intern Med. 2019 Apr 1;179(4):587. doi: 10.1001/jamainternmed.2018.8681. JAMA Intern Med. 2019. PMID: 30933230 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
