

High rates of central obesity and sarcopenia in CKD irrespective of renal replacement therapy - an observational cross-sectional study
- PMID: 30305034
- PMCID: PMC6180401
- DOI: 10.1186/s12882-018-1055-6
High rates of central obesity and sarcopenia in CKD irrespective of renal replacement therapy - an observational cross-sectional study
Erratum in
-
Correction to: High rates of central obesity and sarcopenia in CKD irrespective of renal replacement therapy - an observational cross-sectional study.BMC Nephrol. 2018 Dec 24;19(1):375. doi: 10.1186/s12882-018-1149-1. BMC Nephrol. 2018. PMID: 30583718 Free PMC article.
Abstract
Background: Poor nutritional status of patients with renal disease has been associated with worsening of renal function and poor health outcomes. Simply measuring weight and height for calculation of the body mass index does however not capture the true picture of nutritional status in these patients. Therefore, we measured nutritional status by BMI, body composition, waist circumference, dietary intake and nutritional screening in three groups of renal patients.
Methods: Patients with chronic kidney disease not on renal replacement therapy (CKD stages 3-5, n = 112), after renal transplantation (n = 72) and patients treated with hemodialysis (n = 24) were recruited in a tertiary hospital in Bergen, Norway in a cross-sectional observational study. Dietary intake was assessed by a single 24 h recall. All patients underwent nutritional screening, anthropometric measurements, body composition measurement andfunctional measurements (hand grip strength). The prevalence of overweight and obesity, central obesity, sarcopenia, sarcopenic obesity and nutritional risk was calculated.
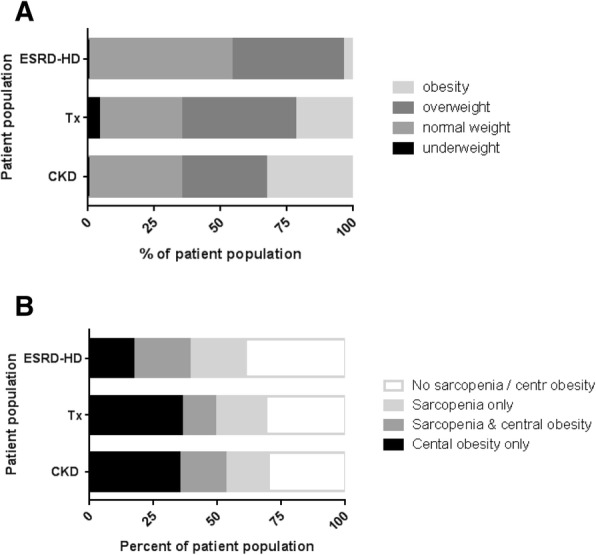
Results: Central obesity and sarcopenia were present in 49% and 35% of patients, respectively. 49% of patients with central obesity were normal weight or overweight according to their BMI. Factors associated with central obesity were a diagnosis of diabetes and increased fat mass, while factors associated with sarcopenia were age, female gender, number of medications. An increase in the BMI was associated with lower risk for sarcopenia.
Conclusion: Central obesity and sarcopenia were present in renal patients at all disease stages. More attention to these unfavorable nutritional states is warranted in these patients.
Keywords: ESRD; Nutritional status; Renal disease; Sarcopenia.
Conflict of interest statement
Ethics approval and consent to participate
The study was conducted in accordance with principles of the Declaration of Helsinki and was approved by the Regional Committee for Medical and Health Research Ethics (REK Vest, (regionale komiteer for medisinik og helsefaglig forskningsetikk, University of Bergen, No. 2014/1790). All patients signed an informed consent prior to participation.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests. The results presented in this paper have not been published elsewhere in whole or in part, except in abstract form.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
