

Prevalence, socio-demographic characteristics, and comorbid health conditions in pre-dialysis chronic kidney disease: results from the Manitoba chronic kidney disease cohort
- PMID: 30305038
- PMCID: PMC6180583
- DOI: 10.1186/s12882-018-1058-3
Prevalence, socio-demographic characteristics, and comorbid health conditions in pre-dialysis chronic kidney disease: results from the Manitoba chronic kidney disease cohort
Abstract
Background: Chronic Kidney Disease (CKD) is common and its prevalence has increased steadily over several decades. Monitoring of rates and severity of CKD across populations is critical for policy development and resource planning. Administrative health data alone has insufficient sensitivity for this purpose, therefore utilizing population level laboratory data and novel methodology is required for population-based surveillance. The aims of this study include a) develop the Manitoba CKD Cohort, b) estimate CKD prevalence, c) identify individuals at high risk of progression to kidney failure and d) determine rates of comorbid health conditions.
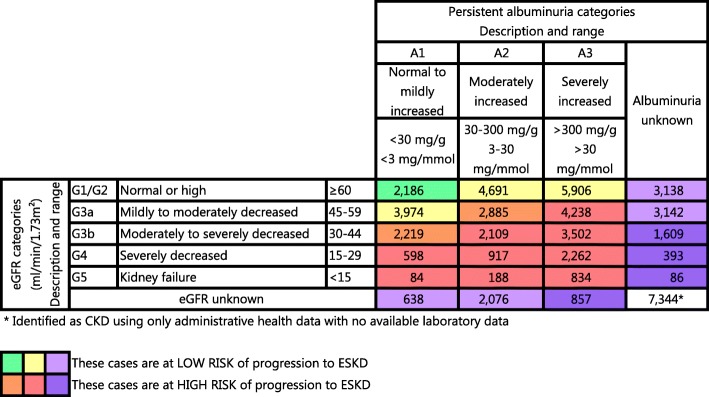
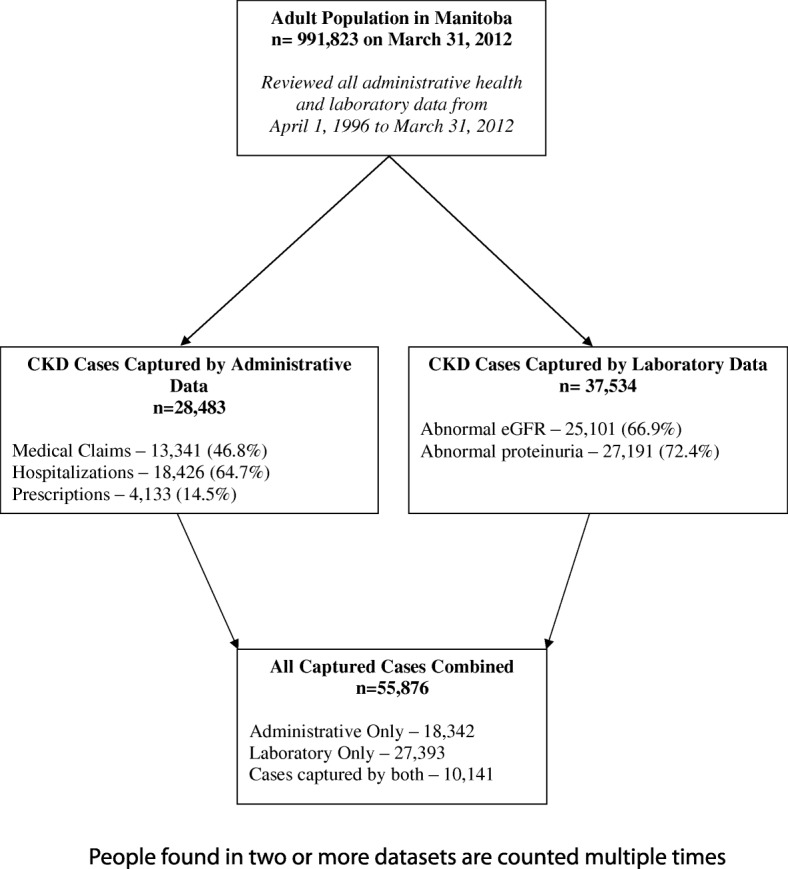
Methods: Administrative health and laboratory data from April 1996 to March 2012 were linked from the data repository at the Manitoba Centre for Health Policy. Prevalence was estimated using three methods: a) all CKD cases in administrative and laboratory databases; b) all CKD cases captured only through the laboratory data; c) and the capture-recapture method. Patients were stratified by risk by estimated Glomerular Filtration Rate (eGFR) and albuminuria based on Kidney Disease Improving Global Outcomes (KDIGO) criteria. For comorbid health conditions, the counts were modelled using a Generalized Linear Model (GLM).
Results: The Manitoba CKD Cohort consisted of 55,876 people with CKD. Of these, 18,342 were identified using administrative health data, 27,393 with laboratory data, and 10,141 people were identified in both databases. The CKD prevalence was 5.6% using the standard definition, 10.6% using only people captured by the laboratory data and 10.6% using the capture-recapture method. Of the identified cases, 46% were at high risk of progression to end-stage kidney disease (ESKD), 41% were at low risk and 13% were not classified, due to unavailable laboratory data. High risk cases had a higher burden of comorbid conditions.
Conclusion: This study reports a novel methodology for population based CKD surveillance utilizing a combination of administrative health and laboratory data. High rates of CKD at risk of progression to ESKD have been identified with this approach. Given the high rates of comorbidity and associated healthcare costs, these data can be used to develop a targeted and comprehensive public health surveillance strategy that encompass a range of interrelated chronic diseases.
Keywords: Administrative data; Chronic kidney disease; Cohort; Comorbidity; Epidemiology; Prevalence; Surveillance.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Health Research Ethics Board (HREB) at the University of Manitoba (HREB#: H2012;297). Obtaining consent for use of administrative databases has been waived by HREB.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Canadian Institute for Health Information (CIHI). Canadian organ replacement register annual report: treatment of end-stage organ failure in Canada, 2004 to 2013. Author. 2015. https://secure.cihi.ca/free_products/2015_CORR_AnnualReport_ENweb.pdf. Accessed 31 Jul 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
