

Association between diuretics and successful discontinuation of continuous renal replacement therapy in critically ill patients with acute kidney injury
- PMID: 30305122
- PMCID: PMC6180655
- DOI: 10.1186/s13054-018-2192-9
Association between diuretics and successful discontinuation of continuous renal replacement therapy in critically ill patients with acute kidney injury
Abstract
Background: Despite aggressive application of continuous renal replacement therapy (CRRT) in critically ill patients with acute kidney injury (AKI), there is no consensus on diuretic therapy when discontinuation of CRRT is attempted. The effect of diuretics on discontinuation of CRRT in critically ill patients was evaluated.
Methods: This retrospective cohort study enrolled 1176 adult patients who survived for more than 3 days after discontinuing CRRT between 2009 and 2014. Patients were categorized depending on the re-initiation of renal replacement therapy within 3 days after discontinuing CRRT or use of diuretics. Changes in urine output (UO) and renal function after discontinuing CRRT were outcomes. Predictive factors for successful discontinuation of CRRT were also analyzed.
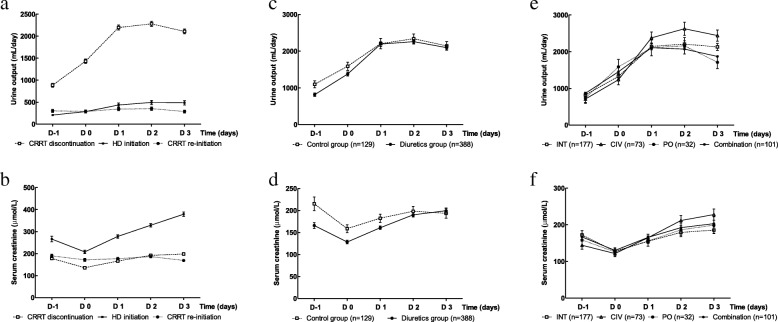
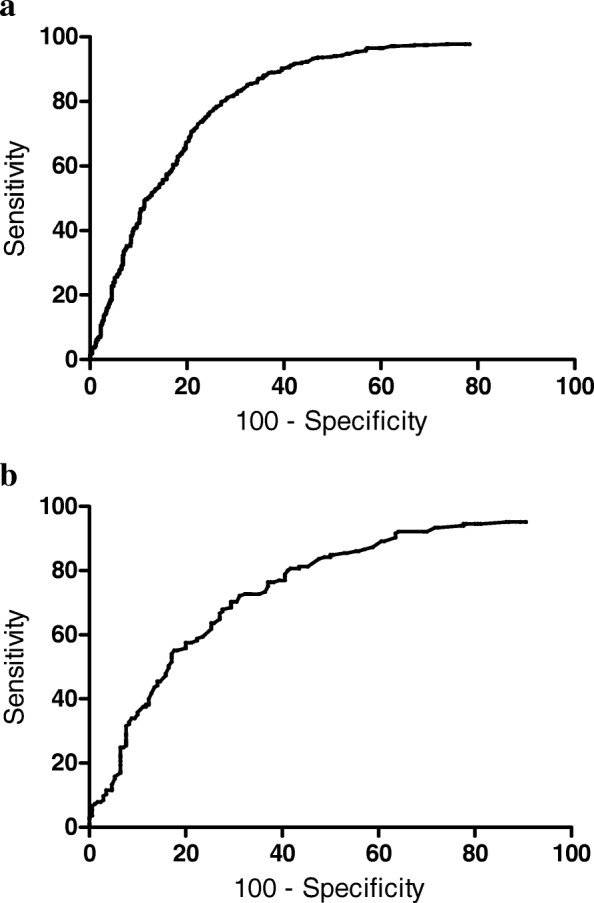
Results: The CRRT discontinuation group had a shorter duration of CRRT, more frequent use of diuretics after discontinuing CRRT, and greater UO on the day before CRRT discontinuation [day minus 1 (day - 1)]. The diuretics group had greater increases in UO and serum creatinine elevation after discontinuing CRRT. In the CRRT discontinuation group, continuous infusion of furosemide tended to increase UO more effectively. Multivariable regression analysis identified high day - 1 UO and use of diuretics as significant predictors of successful discontinuation of CRRT. Day - 1 UO of 125 mL/day was the cutoff value for predicting successful discontinuation of CRRT in oliguric patients treated with diuretics following CRRT.
Conclusions: Day - 1 UO and aggressive diuretic therapy were associated with successful CRRT discontinuation. Diuretic therapy may be helpful when attempting CRRT discontinuation in critically ill patients with AKI, by inducing a favorable fluid balance, especially in oliguric patients.
Keywords: Acute kidney injury; Continuous renal replacement therapy; Diuretics.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of Samsung Medical Center in compliance with the Declaration of Helsinki (IRB number 201510110). No consent for patient participation was needed.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
The furosemide stress test predicts successful discontinuation of continuous renal replacement therapy in critically ill patients with acute kidney injury.J Crit Care. 2025 Feb;85:154929. doi: 10.1016/j.jcrc.2024.154929. Epub 2024 Oct 9. J Crit Care. 2025. PMID: 39383593
-
Early initiation of continuous renal replacement therapy improves survival of elderly patients with acute kidney injury: a multicenter prospective cohort study.Crit Care. 2016 Aug 16;20(1):260. doi: 10.1186/s13054-016-1437-8. Crit Care. 2016. PMID: 27526933 Free PMC article.
-
The Effect of Serum Neutrophil Gelatinase-Associated Lipocalin on the Discontinuation of Continuous Renal Replacement Therapy in Critically Ill Patients with Acute Kidney Injury.Blood Purif. 2019;48(1):10-17. doi: 10.1159/000499026. Epub 2019 Mar 7. Blood Purif. 2019. PMID: 30844791
-
Predictive Factors for the Discontinuation of Renal Replacement Therapy in Critically Ill Adults: A Systematic Review and Meta-Analysis.Cureus. 2025 Apr 6;17(4):e81783. doi: 10.7759/cureus.81783. eCollection 2025 Apr. Cureus. 2025. PMID: 40330386 Free PMC article. Review.
-
Predictors for short-term successful weaning from continuous renal replacement therapy: a systematic review and meta-analysis.Ren Fail. 2023 Dec;45(1):2176170. doi: 10.1080/0886022X.2023.2176170. Ren Fail. 2023. PMID: 36762988 Free PMC article.
Cited by
-
Predictors of 90-Day Restart of Renal Replacement Therapy after Discontinuation of Continuous Renal Replacement Therapy, a Prospective Multicenter Study.Blood Purif. 2019;48(3):243-252. doi: 10.1159/000501387. Epub 2019 Jul 22. Blood Purif. 2019. PMID: 31330511 Free PMC article.
-
Spontaneous diuresis in combination with furosemide stress test (SD-FST) as predictor for successful liberation from kidney replacement therapy: a prospective observational study.Crit Care. 2025 May 26;29(1):214. doi: 10.1186/s13054-025-05452-1. Crit Care. 2025. PMID: 40420285 Free PMC article.
-
Liberation from continuous renal replacement therapy due to renal recovery in adults and children: a literature review and Delphi consensus on clinical practice.Crit Care. 2025 Jul 8;29(1):287. doi: 10.1186/s13054-025-05517-1. Crit Care. 2025. PMID: 40629374 Free PMC article. Review.
-
Different Roles of Functional and Structural Renal Markers Measured at Discontinuation of Renal Replacement Therapy for Acute Kidney Injury.Blood Purif. 2023;52(9-10):786-792. doi: 10.1159/000532034. Epub 2023 Sep 27. Blood Purif. 2023. PMID: 37757763 Free PMC article.
-
Determining the optimal time for liberation from renal replacement therapy in critically ill patients: a systematic review and meta-analysis (DOnE RRT).Crit Care. 2020 Feb 13;24(1):50. doi: 10.1186/s13054-020-2751-8. Crit Care. 2020. PMID: 32054522 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
