

Clinical outcomes of image-guided proton therapy for histologically confirmed stage I non-small cell lung cancer
- PMID: 30305125
- PMCID: PMC6180633
- DOI: 10.1186/s13014-018-1144-5
Clinical outcomes of image-guided proton therapy for histologically confirmed stage I non-small cell lung cancer
Abstract
Background: Two prospective phase II trials were designed to assess the efficacy and safety of image-guided proton therapy (IGPT) for either medically inoperable or operable stage I non-small cell lung cancer (NSCLC). The present study reports the interim results of these trials.
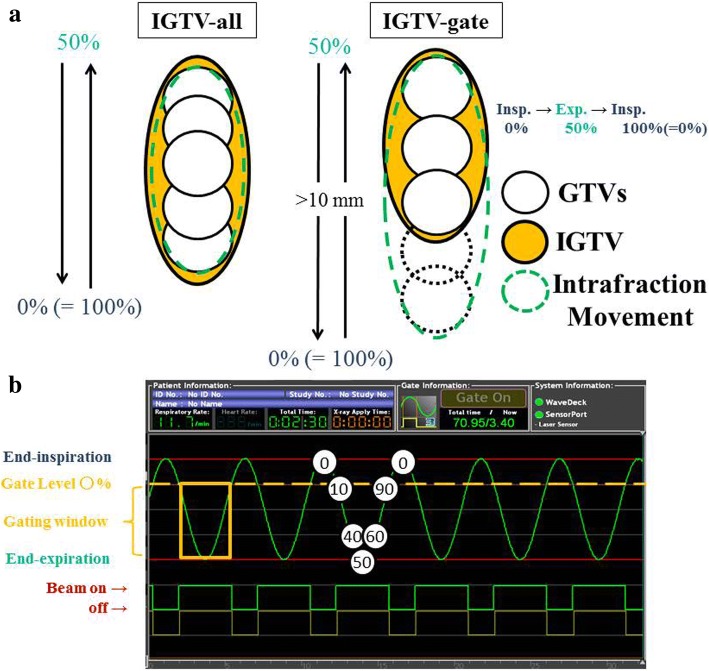
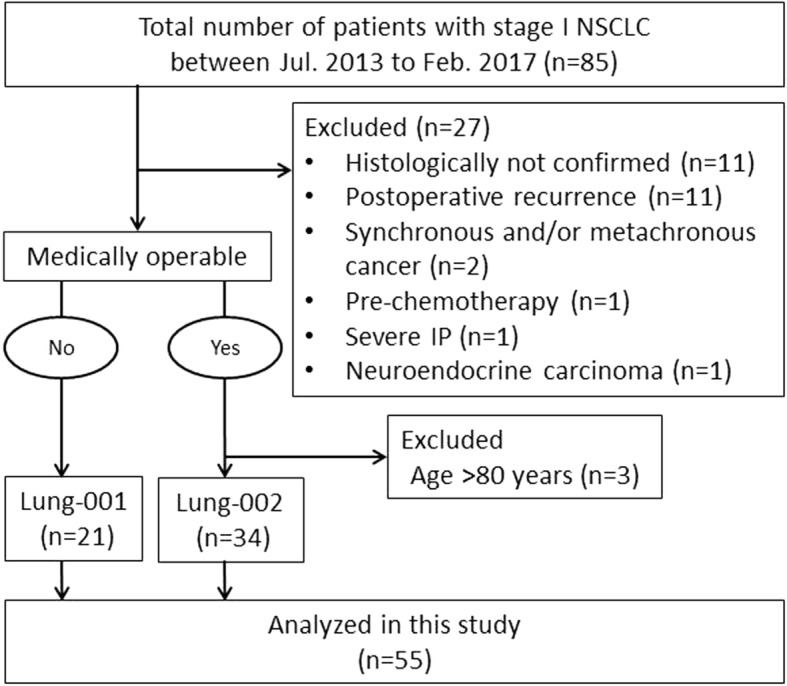
Methods: Fifty-five patients with histologically confirmed stage I NSCLC (IA in 33 patients and IB in 22 patients; inoperable in 21 patients and operable in 34 patients) who received IGPT between July 2013 and February 2017 were analyzed. The median patient age was 71 years (range: 48-88 years). IGPT with fiducial metallic marker matching was performed for suitable patients, and a respiratory gating method for motion management was used for all treatments. Peripherally located tumors were treated with 66 Gy relative biological effectiveness equivalents (Gy(RBE)) in 10 fractions (n = 49) and centrally located tumors were treated with 72.6 Gy(RBE) in 22 fractions (n = 6). Treatment associated toxicities were evaluated using Common Toxicity Criteria for Adverse Events (v.4.0).
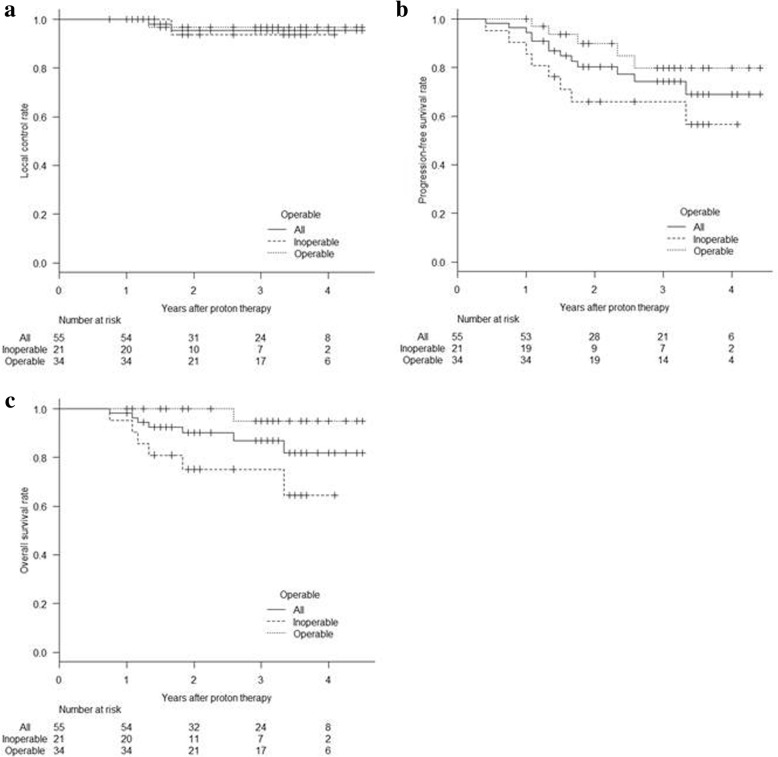
Results: Median follow-up was 35 months (range: 12-54 months) for survivors. For all patients, the 3-year overall survival, progression-free survival, and local control rates were 87% (95% confidence interval: 73-94%), 74% (58-85%), and 96% (83-99%), respectively. Fiducial marker matching was used in 39 patients (71%). Grade 2 toxicities observed were radiation pneumonitis in 5 patients (9%), rib fracture in 2 (4%), and chest wall pain in 5 (9%). There were no grade 3 or higher acute or late toxicities.
Conclusions: IGPT appears to be effective and well tolerated for all patients with stage I NSCLC.
Trial registration: Lung-001, 13-02-09 (9), registered 11 June 2013 and Lung-002, 13-02-10 (10), registered 11 June 2013.
Keywords: Fiducial metallic marker; Image-guided proton therapy; Proton therapy; Respiratory gating system; Stage I non-small cell lung cancer.
Conflict of interest statement
Ethics approval and consent to participate
The data of this study was extracted from ongoing prospective phase II clinical trials based on protocols approved by the Institutional Review Board (IRB) of Nagoya City Hospital. The IRB numbers are 13–02-09 (9) and 13–02-10 (10). Informed consent was obtained from each participant. The study was conducted in accordance with the Declaration of Helsinki.
Consent for publication
We obtained written informed consent to publish the article from patients.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Macdonald OK, Kruse JJ, Miller JM, et al. Proton beam radiotherapy versus three-dimensional conformal stereotactic body radiotherapy in primary peripheral, early-stage non-small-cell lung carcinoma: a comparative dosimetric analysis. Int J Radiat Oncol Biol Phys. 2009;75:950–958. doi: 10.1016/j.ijrobp.2009.04.023. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
