

Increased alloreactive and autoreactive antihuman leucocyte antigen antibodies associated with systemic lupus erythematosus and rheumatoid arthritis
- PMID: 30305912
- PMCID: PMC6173266
- DOI: 10.1136/lupus-2018-000278
Increased alloreactive and autoreactive antihuman leucocyte antigen antibodies associated with systemic lupus erythematosus and rheumatoid arthritis
Abstract
Objectives: Rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) disproportionately affect women during and following childbearing years. Antihuman leucocyte antigen (HLA) alloantibody responses are common in healthy parous women, and as these diseases are both linked with HLA and immune dysregulation, we sought to evaluate anti-HLA antibodies in RA and SLE.
Methods: Anti-HLA antibodies were measured among parous SLE cases (n=224), parous RA cases (n=202) and healthy parous controls (n=239) and compared with each other as well as with nulliparous female and male controls. Antibody specificities were identified and compared against subject HLA types to determine autoreactivity versus alloreactivity. The association of anti-HLA antibodies with clinical outcomes was evaluated.
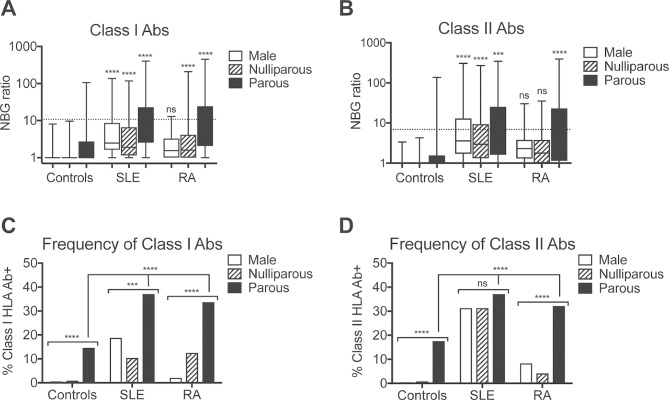
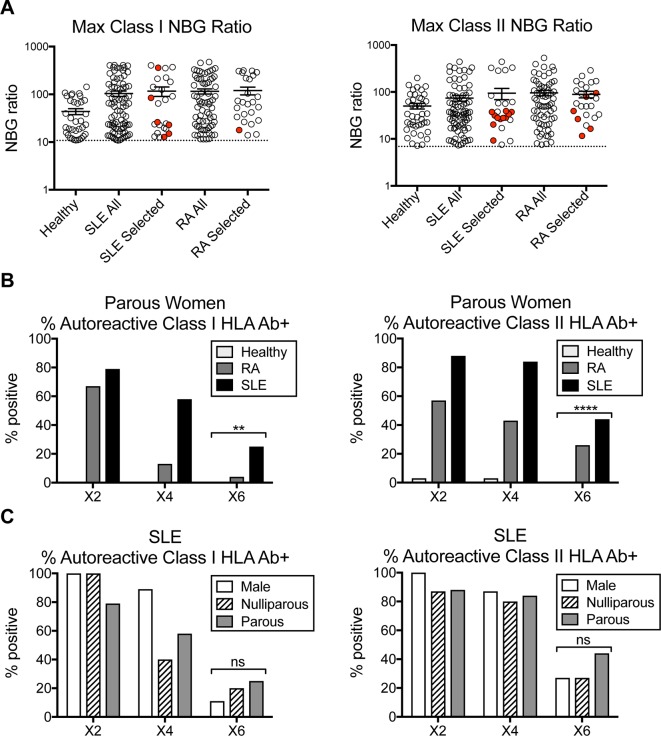
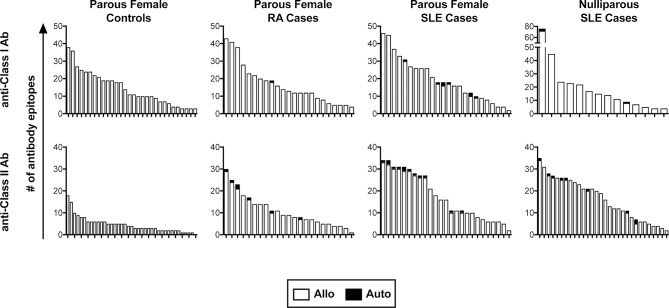
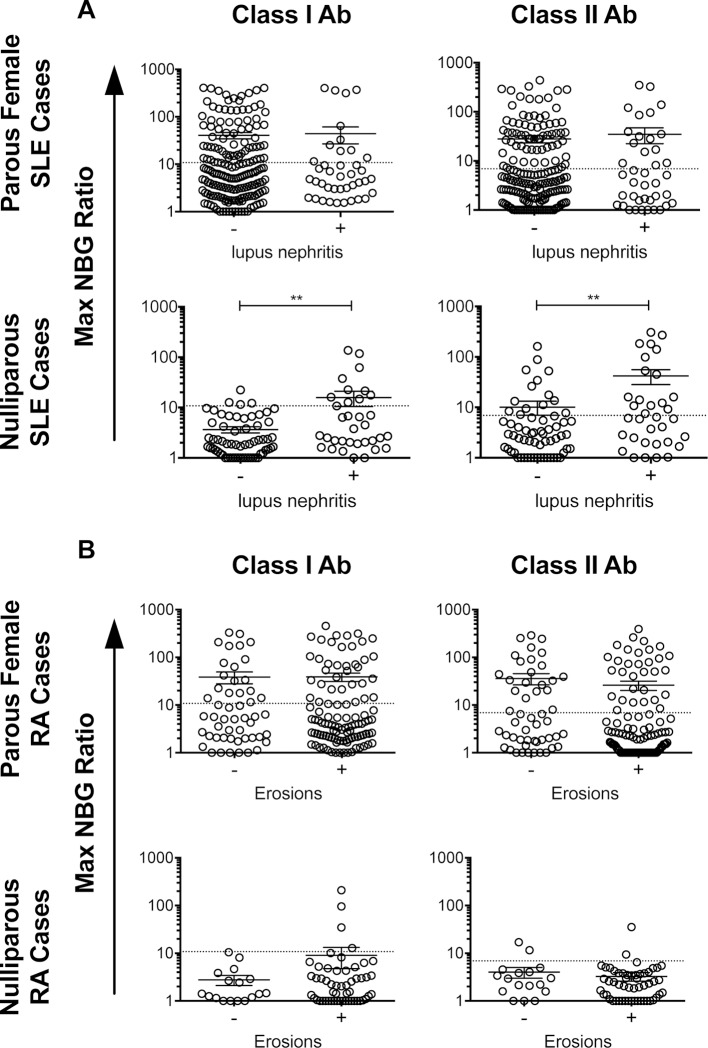
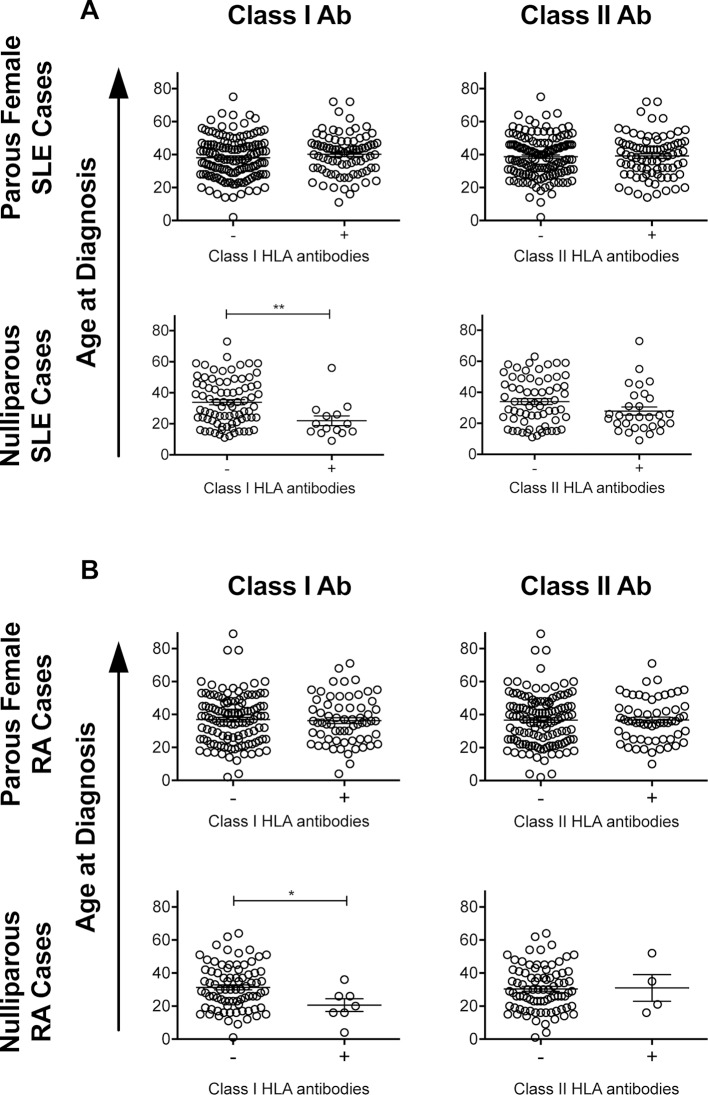
Results: Levels and frequencies of anti-HLA antibodies were significantly higher among parous females with SLE (52%) or RA (46%) compared with controls (26%), and anti-HLA antibodies were also found among nulliparous females and males with SLE and RA. Autoreactive anti-HLA antibodies were observed among SLE and RA antibody-positive subjects, but not healthy controls, with the highest frequency of autoreactive anti-HLA antibodies found in the SLE subjects. Higher levels of anti-HLA antibodies were associated with nephritis among the nulliparous SLE cases (p<0.01). The presence of anti-class I HLA antibodies was associated with younger age at diagnosis among both the RA and SLE nulliparous cases.
Conclusions: Both autoreactive and alloreactive anti-HLA antibodies were found at high levels in RA and SLE subjects. These occurred even in the absence of alloexposure, particularly among SLE subjects and may be linked with disease severity.
Keywords: alloantibodies; autoantibodies; human leukocyte antigen (HLA); rheumatoid arthritis (RA); systemic lupus erythematosus (SLE).
Figures
Similar articles
-
Increased frequency of class I and II anti-human leukocyte antigen antibodies in systemic lupus erythematosus and scleroderma and associated factors: a comparative study.Int J Rheum Dis. 2016 Dec;19(12):1304-1309. doi: 10.1111/1756-185X.12484. Epub 2014 Oct 8. Int J Rheum Dis. 2016. PMID: 25292400
-
Serum Level of Soluble Human Leukocyte Antigen G in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis.Curr Rheumatol Rev. 2023;19(1):64-71. doi: 10.2174/1573397118666220617100226. Curr Rheumatol Rev. 2023. PMID: 35718963
-
Serum antibodies to human leucocyte antigen (HLA)-E, HLA-F and HLA-G in patients with systemic lupus erythematosus (SLE) during disease flares: Clinical relevance of HLA-F autoantibodies.Clin Exp Immunol. 2016 Mar;183(3):326-40. doi: 10.1111/cei.12724. Epub 2015 Dec 16. Clin Exp Immunol. 2016. PMID: 26440212 Free PMC article.
-
[Anti-cyclic citrullinated peptide antibodies in rheumatoid arthritis: relation with clinical features, cytokines and HLA-DRB1].Biomedica. 2004 Jun;24(2):140-52. Biomedica. 2004. PMID: 15495594 Review. Spanish.
-
Meta-analysis of associations between functional HLA-G polymorphisms and susceptibility to systemic lupus erythematosus and rheumatoid arthritis.Rheumatol Int. 2015 Jun;35(6):953-61. doi: 10.1007/s00296-014-3155-3. Epub 2014 Oct 18. Rheumatol Int. 2015. PMID: 25326335 Review.
Cited by
-
Dysregulated T Cell Activation and Aberrant Cytokine Expression Profile in Systemic Lupus Erythematosus.Mediators Inflamm. 2019 Mar 17;2019:8450947. doi: 10.1155/2019/8450947. eCollection 2019. Mediators Inflamm. 2019. PMID: 31007604 Free PMC article.
-
HLA Homozygosity and Likelihood of Sensitization in Kidney Transplant Candidates.Transplant Direct. 2022 Apr 7;8(5):e1312. doi: 10.1097/TXD.0000000000001312. eCollection 2022 May. Transplant Direct. 2022. PMID: 35415215 Free PMC article.
-
Anti-HLA Class II Antibodies Correlate with C-Reactive Protein Levels in Patients with Rheumatoid Arthritis Associated with Interstitial Lung Disease.Cells. 2020 Mar 11;9(3):691. doi: 10.3390/cells9030691. Cells. 2020. PMID: 32168865 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials