

Anatomy of the atrial septum and interatrial communications
- PMID: 30305943
- PMCID: PMC6174145
- DOI: 10.21037/jtd.2018.02.18
Anatomy of the atrial septum and interatrial communications
Abstract
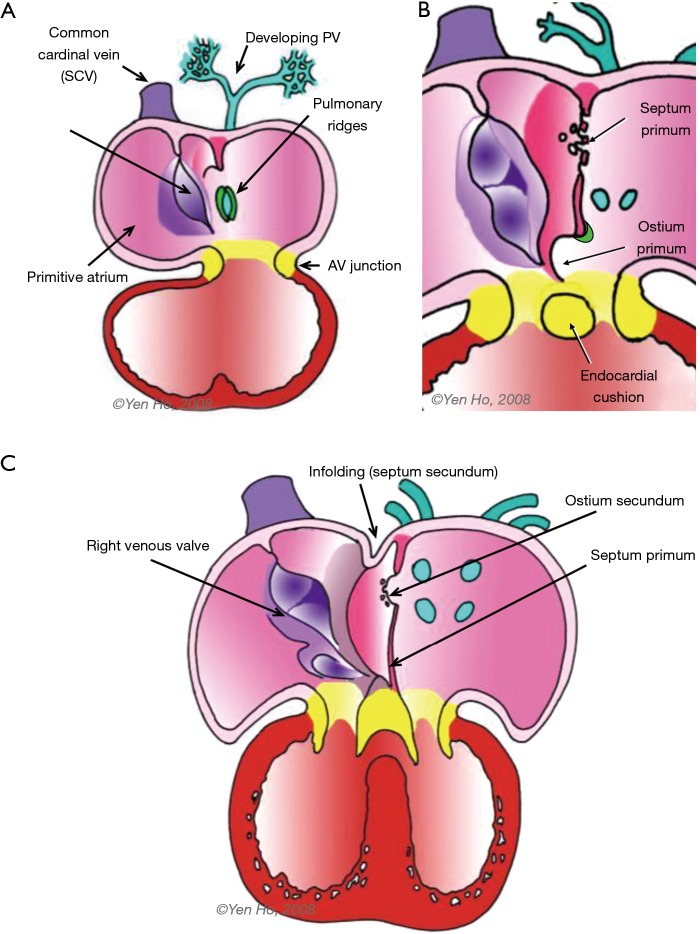
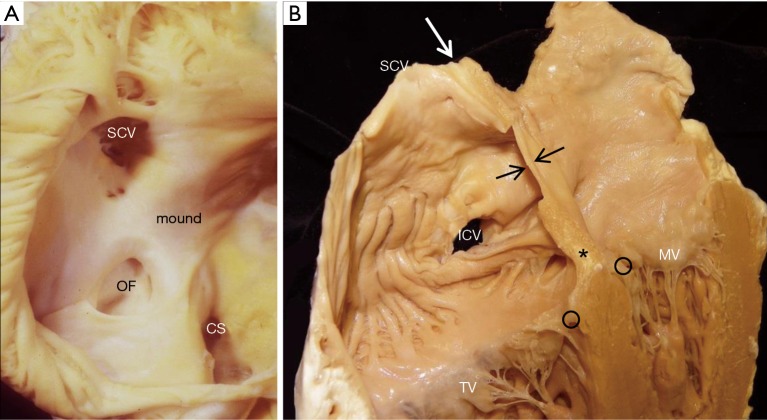
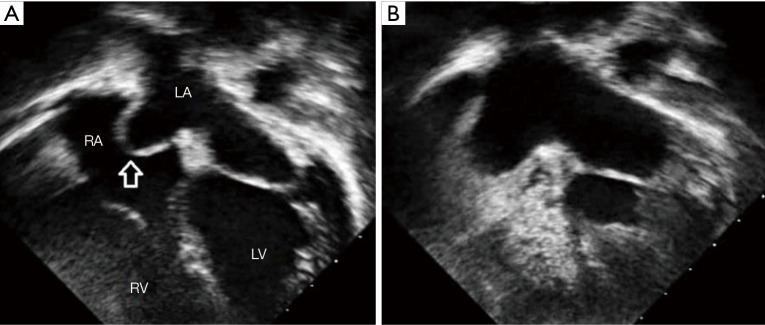
Deficiencies in the septum separating the two atrial chambers are among the most common of congenital heart malformations. This article reviews the developmental aspects of the partitioning of the primitive atrium into right and left atrial chambers, the anatomical components of the atrial septum, and deficiencies that produce the various types of interatrial communications. Knowledge of the components of the true atrial septum in the developed heart clarifies the morphology of various types of interatrial communications. The oval fossa defect (also termed secundum ASD) is located within the true septum. The patent foramen ovale (PFO) is a tunnel-like passageway between the free edge of the overlapping ovale fossa valve and its muscular rim. Other defects such as superior and inferior sinus venosus defects, coronary sinus defects, and ostium primum defects lie outside the area of the true septum.
Keywords: Atrial septal defect (ASD); coronary sinus defect; patent foramen ovale (PFO); sinus venosus defect.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures





References
-
- van der Linde D, Konings EE, Slager MA, et al. Birth prevalence of congenital heart disease worldwide. A systematic review and meta-analysis. J Am Coll Cardiol 2011;58:2241-7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources